Judgment and Decision Making, Vol. 15, No. 4, July 2020, pp. 572-585
Are the symptoms really remitting? How the subjective interpretation of outcomes can produce an illusion of causality
Fernando Blanco*
Maria Manuela Moreno-Fernández#
Helena Matute#
|
Judgments of a treatment’s effectiveness are usually biased by the
probability with which the outcome (e.g., symptom relief) appears: even
when the treatment is completely ineffective (i.e., there is a null
contingency between cause and outcome), judgments tend to be higher when
outcomes appear with high probability. In this research, we present
ambiguous stimuli, expecting to find individual differences in the
tendency to interpret them as outcomes. In Experiment 1, judgments of
effectiveness of a completely ineffective treatment increased with the
spontaneous tendency of participants to interpret ambiguous stimuli as
outcome occurrences (i.e., healings). In Experiment 2, this interpretation
bias was affected by the overall treatment-outcome contingency, suggesting
that the tendency to interpret ambiguous stimuli as outcomes is learned
and context-dependent. In conclusion, we show that, to understand how
judgments of effectiveness are affected by outcome probability, we need to
also take into account the variable tendency of people to interpret
ambiguous information as outcome occurrences.
Keywords: illusion of causality, outcome-density, contingency learning
1 Introduction
Most decisions that we make every day are based on causal knowledge. For
example, we could take a painkiller because we think that it will help us
reduce our headache; or we could use the seatbelt when driving, in the
belief that it will prevent damage in case of car accident. These are
decisions that imply a causal link between two types of events: causes
(taking a pill, using the seatbelt) and effects or outcomes (symptomatic
relief, damage prevention). Since decisions of this kind could be of high
relevance for our survival or quality of life, it would be desirable that
the causal beliefs that guide them are accurate. However, as we will later
explain, this is not always the case: people could insist on taking a
completely ineffective treatment (pseudomedicine) because they erroneously
believe it has beneficial effects; or they could decide not to use the
seatbelt because they fail to see the preventive causal link between this
safety measure and accidental damage. Thus, it is important to conduct
research on how causal knowledge can be biased, and on the individual
differences that explain why some people could be more prone to errors.
In this research endeavor, we need first to address how causal beliefs are
formed through the process of causal learning. This often involves
learning the contingency, or statistical correlation, between the
potential cause and the outcome. One of the many ways in which this
contingency information can be obtained is from the direct experience with
both events. For the simplest case, with only one cause and one outcome,
and assuming that both variables are binary (either they occur or they do
not), there are four possible events that one can experience: type a
trials (both the cause and the outcome occur), type b trials (the cause
occurs, but the outcome does not), type c trials (the cause, but not the
outcome, occurs), and type d trials (neither occurs). These types of trial
(a, b, c, and d) could appear with different frequencies. One could use
this information to compute an index of contingency, such as Δ P
(Allan, 1980; see alternative rules in Perales & Shanks, 2007):
|
Δ P = P(O|C)−P(O|¬ C) = | | − | |
(1) |
As Equation 1 shows, the index assesses the difference between two
conditional probabilities: the probability of the outcome conditional on
the presence of the cause, P(O|C), and the probability of the
outcome conditional on the absence of the cause, P(O|¬ C). If
the outcome is more likely to appear in the presence of the potential
cause than it is in the absence of the potential cause, then the Δ
P index will take a positive value, indicating that there is some degree
of contingency between the two events, and suggesting a causal link. For
example, if a given food item produces allergic symptoms, one would
observe that the allergic reaction appears more often after taking the
food than after not taking it. A negative value of Δ P indicates
the opposite relationship: P(O|C) is smaller than
P(O|¬ C). For example, the probability of serious damage in
case of car accident is smaller when one uses the seatbelt than when one
does not. Finally, and what is more relevant for our study, there are
situations in which both probabilities are equal, thus yielding a Δ
P value of 0. This is a null contingency setting that normally implies
the absence of a causal link. For example, using a pseudoscientific
treatment for a serious disease will probably not improve the chances of
healing as compared to when no treatment, or a placebo, is taken (Yarritu,
Matute & Luque, 2015).
A great deal of evidence indicates that people (and other animals) are
capable of detecting contingency, and that they can use this information
for making causal judgments and decisions (Baker, Mercier,
Vallée-Tourangeau & Frank, 1993; Blanco, Matute & Vadillo, 2010;
Rescorla, 1968; Shanks & Dickinson, 1988; Wasserman, 1990). However,
research has documented some factors that bias contingency estimations,
particularly in null contingency settings. Perhaps the most widely studied
of these biases is the outcome-density effect (OD): Given a fixed (usually
null) contingency value, judgments will systematically increase above zero
when the marginal probability of the outcome, P(O), is high, compared to
when it is low (Alloy & Abramson, 1979; Buehner, Cheng & Clifford,
2003; Moreno-Fernández, Blanco & Matute, 2017; Musca, Vadillo, Blanco
& Matute, 2010). This is a robust effect that has been replicated, and
that could lead to causal illusions (perception of causal links in
situations in which there is none; see for review Matute et al., 2015;
Matute, Blanco & Díaz-Lago, 2019). These mistaken beliefs could, in
turn, entail serious consequences, as they could underlie illusions of
effectiveness of pseudoscientific medicine (Matute, Yarritu & Vadillo,
2011), and contribute to maintain social prejudice (Blanco, Gómez-Fortes,
& Matute, 2018; Rodríguez-Ferreiro & Barberia, 2017).
Given the importance of understanding both accurate and biased contingency
detection to make sense of people’s causal beliefs and decisions, it would
be useful to find out whether some individuals are more likely to bias
their judgments than others. Consequently, many researchers in the field
of contingency learning have shifted their interest toward finding
evidence for individual differences in contingency detection (Byrom, 2013;
Byrom & Murphy, 2017; Sauce & Matzel, 2013). Thus, we know that people
differ in their sensitivity to the OD effect. For example, while the OD
bias seems quite prevalent in the general population, people with mild
dysphoria are more resistant to this manipulation (i.e., depressive
realism, Alloy & Abramson, 1979; Msetfi, Murphy & Simpson, 2007).
Believers in the paranormal can also show stronger OD biases when facing a
contingency learning task on an unrelated domain (Blanco, Barberia &
Matute, 2015; Griffiths, Shehabi, Murphy & Le Pelley, 2018).
Additionally, people can selectively display a stronger/weaker OD bias
depending on the content of the materials, and how it
contradicts/reaffirms their previous attitudes (Blanco et al., 2018).
Finally, even more subtle differences such as assuming a higher or lower
base-rate for the outcome can in fact modulate the OD bias, making it
stronger or weaker, because the actual P(O) observed during the experiment
can be interpreted as high or low depending on the one that was previously
assumed (Blanco & Matute, 2019).
1.0.1 When the OD (outcome-density) bias depends on our interpretation
The study we have just mentioned (Blanco & Matute, 2019) illustrates that
people who receive identical or similar information (a null contingency
made up of a sequence of type a, b, c, and d trials) can produce weaker OD
biases when they interpret that the P(O) they observed is actually lower
than the one they should expect (Experiment 1). Additionally, they also
would produce the opposite, stronger OD biases, when they judge that the
P(O) they saw is higher than they were expecting (Experiment 2). That is,
not only the actual level of P(O) matters for developing the OD bias, but
the interpretation that the participant makes is also important.
This opens the question of whether all people tend to interpret outcome
occurrences in the same way, when it comes to learning a contingency or
grasping a potential causal relationship. In real life, it is often not
clear when an outcome has occurred. Consider a person who is treating
his/her common cold with a treatment. At the beginning of the treatment,
the symptoms are intense and easy to recognize. However, as the disease
resolves and health improves, symptoms become less severe, making them
sometimes difficult to detect or categorize as such: If I cough less
frequently today than I did yesterday, I could either interpret it as a
healing (i.e., an outcome occurrence), or instead focus on the fact that I
am still coughing, so I am not completely healed (that is, a no-outcome
trial). Note that depending on my interpretation of what counts as an
outcome, the overall P(O) that I will experience will likely be very
different, and the contingency may also be affected. Thus, the
interpretation of outcome information can in fact determine the judgment
of causality (in this case, the judgment about the effectiveness of the
treatment). Therefore, this could be a potential source of individual
variability in the sensitivity to the OD bias: given the same level of
actual P(O), people might produce very different judgments of causality
because of their interpretations of outcome events.
If different interpretations of outcome events are possible, it is because,
in real life, many relevant outcomes are usually continuous (i.e., they are
a matter of degree) and variable. By contrast, in the great majority of
experiments, they are binary (they either occur or not) and fixed. A recent
exception are the studies conducted by Chow and colleagues (Chow, Colagiuri
& Livesey, 2019). In their experiments, participants rated how effective a
medicine was, after seeing a series of trials in which the medicine and the
outcome (healing) could either be present or not (i.e., the four trial
types described above), as it is common in the literature on this
topic. However, instead of presenting outcome information in a binary
fashion (i.e., “present”/“absent”), they conveyed this information as a
number describing the “health level” of the patient, thus creating the
impression that outcomes were continuous. Additionally, trials defined as
outcome-present did not always depict exactly the same health level.
Instead, some random variation was added (i.e., the outcomes were variable
rather than fixed). This is a more ecological setting than previously used
ones, as many real-life situations (such as judging whether a treatment is
working for a common cold) can be better thought as involving continuous
and variable outcomes. Although this type of presentation implies that the
task becomes more difficult (i.e., it is harder to ascertain whether the
outcome took place or not, or whether our health is actually improving or
not, if the outcome takes an intermediate value), the results clearly
indicated that the OD bias appears systematically, with similar size, both
in binary-fixed outcome conditions and in continuous-variable outcome
conditions.
It has been hypothesized (Chow et al., 2019; Marsh & Ahn, 2009) that, when
presented with the information of a continuous outcome, people
spontaneously categorize this information into one of the four categories
(type a, b, c, and d trials). That is, despite the information is
continuous, the usual interpretation by the participant reduces it to a
discrete value (either the event took place or not). Chow et al.’s (2019)
study did not consider potential differences between participants in their
tendency to classify a given outcome value as an outcome
occurrence/absence, since this was not the aim of their research. However,
as we illustrated above, these differences could exist in real-life
situations involving continuous and variable outcomes (because they can be
interpreted in various ways). For example, some people would subjectively
interpret their 10% symptomatic remission as an outcome (i.e., healing),
while others would make the opposite classification because 10% is too
small a change.
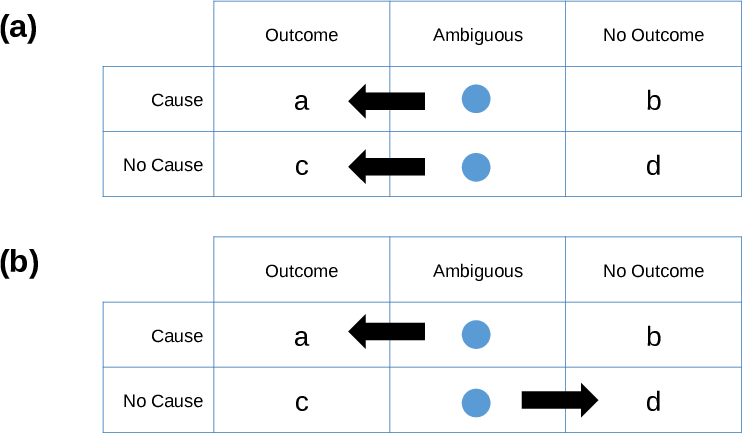
| Figure 1: Two ways in which individual differences in the interpretation of
ambiguous stimuli could lead to illusions of effectiveness (overestimated
judgments of causality): either (a) by systematically categorizing
ambiguous stimuli as outcomes (cells a and c), therefore inflating P(O),
or (b) by inflating the contingency through the differential
categorization of ambiguous stimuli as outcome or no outcome, depending on
the presence of the cause, that is, cells a and d. |
In this task of interpreting and classifying outcomes, perceptual processes
may play an important role, as they are key to discriminating different
stimuli (in this case, “outcome” vs. “no outcome”). In fact, individual
differences in the tendency to detect meaningful patterns in ambiguous
perceptual material have been widely documented. For example, people who
believe in the supernatural and in conspiracy theories are more likely to
illusorily perceive a meaningful pattern in a stimulus consisting of
random clouds of dots (van Elk, 2015; van Prooijen, Douglas & De
Inocencio, 2017), as it happens too to participants who feel lack of
control (Whitson & Galinsky, 2008; although see Van Elk & Lodder, 2018).
Similarly, patients with schizophrenia tend to produce more false-alarm
errors and be overconfident when judging ambiguous visual patterns
(Moritz, Ramdani, et al., 2014), a mechanism that has been linked to
hallucinations and delusions, typical in this disorder. Moreover, both
paranormal beliefs and schizophrenia have been associated to causal
illusions of some kind (Blanco et al., 2015; Moritz, Goritz, et al., 2014;
Moritz, Thompson & Andreou, 2014), including the OD bias, which might
indicate a common underlying mechanism. We suggest that the tendency of
these participants to interpret ambiguous patterns as outcome occurrences,
thus inflating the P(O) they are factually exposed to, might be one key
factor at the basis of their stronger vulnerability to causal illusions.
In this article, we describe two experiments conducted on healthy
individuals. In Experiment 1, our aim was to document individual
variability in the tendency to categorize ambiguous information as outcome
occurrences. This variability could be important, because it can affect
judgments of causality in two different ways: (a) if the tendency to
categorize the stimuli as outcome or no-outcome does not depend on whether
the cause is present, then those people who report perceiving the outcome
more often will not experience an inflated contingency, but will
nevertheless experience an inflated value of P(O) that can lead to
overestimated judgments of causality (OD bias). This possibility is
depicted schematically in Figure 1a. Note that, as the tendency to
interpret the stimuli as outcomes is in this case not affected by the
presence of the cause, the overall perceived contingency remains
unchanged, because a similar proportion of ambiguous trials will be
categorized as outcomes when the cause is present and when the cause is
absent. On the other hand, there is a second possibility: (b) If the
tendency to categorize the stimuli as outcomes is different depending on
whether the cause is present or not, then participants will be effectively
experiencing a different contingency from the one that was programmed,
thus leading to judgments that do not match the programmed contingency
(Figure 1b). For instance, people expecting the cause to produce the
outcome might tend to interpret an ambiguous stimulus as an outcome more
often in the presence of the cause than in its absence, which could
increase the perceived contingency beyond its actual value.
In sum, we have two potential ways in which the variability in the
interpretation of ambiguous stimuli could produce causal illusions: by
inflating P(O), or by inflating contingency. We will first investigate
which of the two predictions (Figure 1a or Figure 1b) holds in null
contingency settings, which are the conditions that typically produce
overestimated judgments.
2 Experiment 1
In this experiment, we aim to investigate how differences in the tendency
to interpret ambiguous stimuli as “outcome” or “no outcome” could produce
changes in the causal judgments. Specifically, individuals with a more
liberal criterion (i.e., most stimuli are categorized as “outcome”) would
experience a high subjective P(O), which would result in strong
overestimations of a null contingency (OD bias). This would contrast with
participants with a more conservative criterion, who would display the
opposite pattern. In principle, we assume that there will not be
differences in the outcome interpretation criterion depending on the
presence of the cause (in line with the prediction of Figure 1a), because
there is no a priori reason to expect that outcomes should appear with
different probabilities depending on the cause status.
2.1 Method
2.1.1 Participants and apparatus
One hundred Psychology students (out of which 19 men) from the University
of Deusto took part in Experiment 1 in exchange for course credit (with age
M = 18.50 years, SD = 0.86). The experiment was conducted
in a large computer room. All materials were presented in Spanish. The
experimental task was implemented as a JavaScript program that can
run online in most browsers, without installing any plugin or additional
programs. The
participants were informed before the experiment that they could quit the
study at any moment by closing the browser window. The data collected
during the experiment were sent anonymously to the experimenter only upon
explicit permission by the participant, indicated by clicking on a
“Submit” button. If the participant clicked on the “Cancel” button, the
local information was erased. No personal information (i.e., name, IP
address, e-mail) was collected. We did not use cookies or other software to
covertly obtain information from the participants.
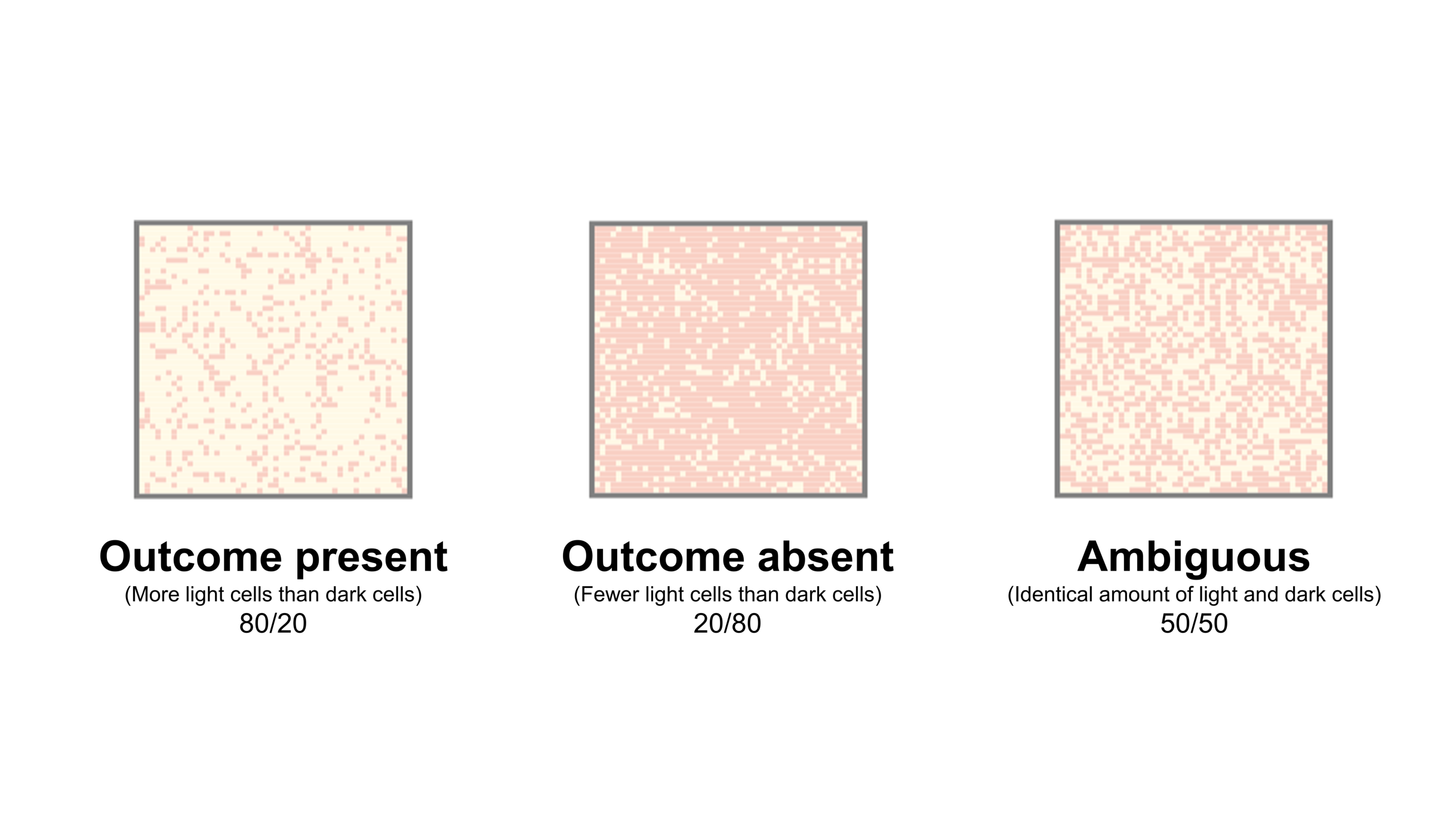
| Figure 2: Examples of stimuli used in outcome-present trials (cured
patient), outcome-absent trials (no cured patient), and ambiguous trials
in the contingency learning task. Note that the assignment of colors
(light/dark) to roles (ill/normal cells) was randomly decided for each
participant, but for simplicity we present here only one of the
assignments. |
2.1.2 Procedure
Within the Method, overview of the study procedure. The experiment was
designed as a standard trial-by-trial contingency learning task (Matute et
al., 2015), framed in a medical scenario (a fictitious medicine,
Batatrim, plays the role of potential cause, and the recovery
from a disease is the outcome). However, we introduced a number of changes
to adapt the task to our current purposes.
The main innovation in this procedure is in the stimuli used as outcome. On
each trial, the information about the outcome was presented on a 50 x 50
pixels matrix which represents a tissue sample obtained from a given
patient. The matrix contained 2500 points (i.e., cells) of two colors
(dark pink and light yellow), randomly distributed in space. The
proportion of light to dark cells was determined by the type of trial. The
instructions stated that the Lindsay Syndrome (a fictitious disease)
affects human tissues and causes some of the cells to appear in a dark
color, instead of the normal light color. (Note that the assignment of
dark/light colors to ill/normal cells was randomly decided for each
participant, although, for simplicity, in this section we will refer only
to one of the two possible assignments: dark for ill cells, and light for
normal cells.) More specifically, participants were told that: (a) a
patient suffering from the syndrome will present more dark cells than
light cells and, conversely, that (b) when a patient has overcome the
syndrome, his/her tissues will contain more light than dark cells. Thus,
in outcome-present trials (i.e., a and c, when the patient is cured),
there will be 2000 light cells (80%) and 500 dark cells (20%), whereas
in outcome-absent trials (i.e., b and d, when the patient is not cured),
the proportion will be the opposite. These proportions were decided to
make the task of interpreting outcome-present and outcome-absent trials
easy, because the perceptual difference between these two types of trials
is notable (Figure 2, left and center).
To ensure all participants were able to acquire this discrimination
correctly, we included a practice phase in which a series of eight stimuli
with various level of difficulty (i.e., proportions 90/10, 80/20, 70/30,
60/40, 40/60, 30/70, 20/80, and 10/90) had to be categorized as “cured/not
cured” tissue, and the appropriate feedback was then provided. If
participants failed to categorize more than two out of these eight
stimuli, they were forced to continue the practice phase until they
achieved at least six out of eight correct classifications (i.e., 75%).
| Table 1: Frequencies of each type of trial in the contingency learning phase of
Experiment 1. |
| | Outcome present (cured) | Ambiguous Outcome | Outcome absent (not cured) |
| Cause present (Medicine was taken) | 5 | 10 | 5 |
| Cause absent (Medicine was not taken) | 5 | 10 | 5 |
Once the practice phase was over, participants underwent the learning
phase. During the contingency learning phase there was an additional type
of trial, which presented an ambiguous outcome with as many light cells as
dark cells (Figure 2, right). This stimulus (50/50) cannot be objectively
interpreted as cured (outcome) or not cured (no outcome), because it lies
exactly in the middle between cured and not cured tissues. Therefore, there
could be individual differences in interpretation of ambiguous trials:
participants with a conservative criterion would interpret most ambiguous
stimuli as outcome-absent, whereas those with a liberal criterion would
interpret them as outcome-present. Additionally, participants could, to
some extent, tend to categorize the ambiguous stimulus as outcome or not
depending on whether the cause (medicine) is present, as explained in the
Introduction.
Table 1 contains the frequencies of each type of trial presented in the
contingency learning phase. Attending to non-ambiguous trials, the
contingency between taking the medicine and healing was null, since the
probability of overcoming the syndrome was identical both in the presence
and in the absence of the medicine, i.e., P(O|C) = P(O|¬ C) =
0.50. However, the interpretation of ambiguous trials could affect this
computation: for example, if participants tend to categorize or interpret
the ambiguous stimuli as “outcome” more often in the presence of the cause
than in its absence, then the actually perceived contingency would become
positive, P(O|C) > P(O|¬ C) (see, e.g., Figure 1b). The 30 trials were
arranged in random order for each participant.
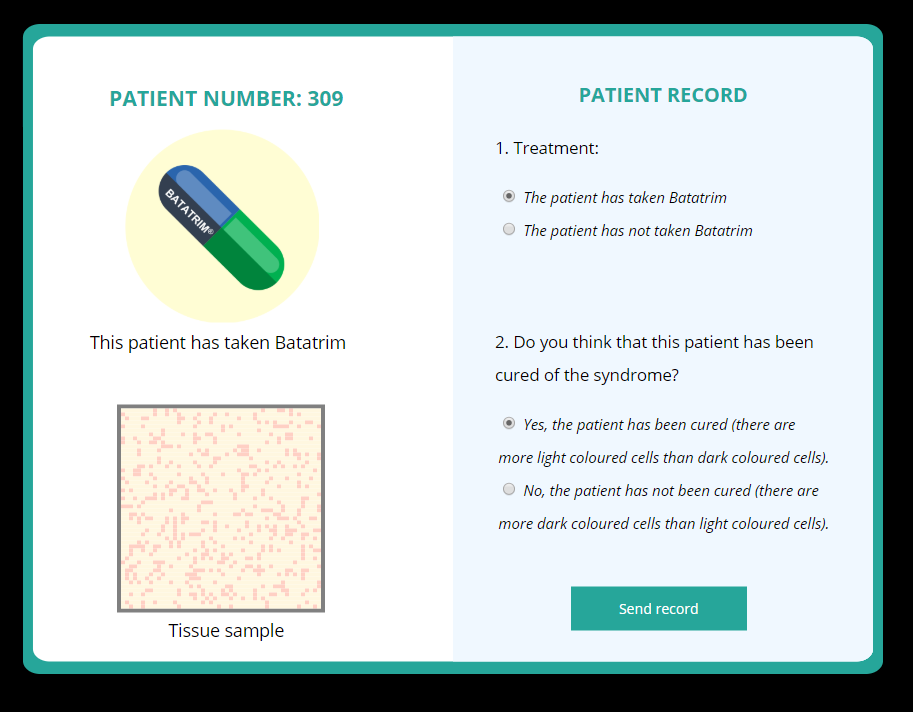
| Figure 3: Screenshot of one trial in the contingency learning task. On the
left-hand of the screen, participants see the information about the cause
and outcome statuses. Then, on the right-hand, they must categorize the
status for both cause and outcome. |
The distribution of non-ambiguous trial frequencies depicted in Table 1 was
chosen to optimize the information provided by our study. Since we aimed
to examine the spontaneous tendency to categorize ambiguous stimuli as
outcomes in a null contingency setting, the frequencies of all four types
of non-ambiguous trials were set to be identical, i.e., P(O) = P(C) =
0.50. This ensures that for all participants, non-ambiguous trials provide
the same information: a null contingency between the cue and the outcome
and a medium level of P(O) and P(C). Any deviation from these
frequencies, such as a P(O) > 0.50, could introduce a bias
as it could affect the tendency to categorize ambiguous stimuli (Experiment
2 will deal with one of these situations).
To assess the tendency to categorize the stimuli, the contingency learning
task included two questions in each trial (see a sample of a trial in
Figure 3). The instructions to this phase asked the participants
to help the researchers classify each record in a fictitious study that
was conducted to test the effectiveness of the medicine. On each trial,
the information about the cause (medicine) and outcome (tissue) appeared
on the left hand of the screen (e.g., “This patient took
Batatrim; This is the tissue sample”). Then, participants had to
indicate, in this order: (a) whether the patient took Batatrim or
not (i.e., thus categorizing the cause status), and then (b) whether the
outcome occurred or not (i.e., thus categorizing the outcome status). A
reminder of the correct interpretation of dark/light cells was provided
(Figure 3) to help in the task, but no feedback was given during this
phase. Although we were interested only in the interpretation of outcomes,
because categorizing the cause status was trivial in this task, we
included both questions to prevent participants from focusing too much on
outcomes and overlook the causes. The responses to the outcome
categorization were recorded for all trials (0: no outcome; 1: outcome),
thus allowing us to compute a subjective P(O) index: the number of
outcomes categorized as “outcome” over the total number of trials.
Additionally, we also computed the subjective contingency index, which is
obtained by applying the Δ P rule to the trial frequencies, after
recoding them according to the categorization (i.e., if the ambiguous
stimulus in a cause-present trial is categorized as “outcome”, then it
counts as a “type a” trial, and so on). Both subjective P(O) and
subjective contingency could affect the perceived contingency between
medicine and healings.
After the sequence of thirty trials, participants were asked to rate the
extent to which the medicine, Batatrim, was able to heal the
syndrome (i.e., a causal judgment), as is typical in these tasks. The
judgment was collected on a scale from 0 (not effective at all) to 50
(quite effective) to 100 (completely effective). Given that the actual
contingency, considering non-ambiguous trials, was set to null, the correct
answer should be zero. However, some participants could show a causal
illusion (i.e., an overestimation of the causal relationship), as revealed
by a higher judgment, as is usual in previous experiments with this type of
task (Alloy & Abramson, 1979)1.
2.2 Results and discussion
2.2.1 Categorization of non-ambiguous stimuli (attention checks)
First, we used the practice phase to ensure participants were able to learn
the categorization rule. All participants were able to successfully meet
the practice phase criterion to continue to the contingency learning phase
at their first attempt (i.e., all answered more than six items correctly):
83% of participants answered all eight practice trials correctly, and
17% missed only one out of eight trials. Then, we examined the number of
mistakes made in the categorization of causes and outcomes in
non-ambiguous trials during the contingency learning phase. Most
participants committed none or few mistakes. When categorizing outcomes in
non-ambiguous trials, 93% of participants did not make any mistake, 99%
made 4 or fewer, and only one participant showed an extreme behavior with
20 mistakes out of 20 non-ambiguous trials. This suggests that this
individual interpreted the task backwards (all outcomes were understood as
no-outcomes and vice versa, despite solving successfully the practice
phase, and probably ignoring all written messages that reminded the
correct meaning of the light/dark cells). In comparison, categorizing the
causes led to more errors, but still 65% of the sample did not make any
mistake, and 95% made 5 or fewer. The task of categorizing the cause
status was actually very easy (i.e., it consisted of just repeating the
information that was still available on the screen, as Figure 3
indicates), but perhaps the focus on outcome categorization drew the
attention away from the cause information, so that participants can
inadvertently click on the wrong answer.
| Table 2: Descriptive statistics for the variables in the contingency learning phase
in Experiment 1. |
| | Non-ambiguous trials | Ambiguous trials | All trials |
|
Variable | M | SD | M | SD | M | SD |
| Subjective P(O) | 0.497 | 0.023 | 0.430 | 0.377 | 0.464 | 0.189 |
| Subjective P(O|C) | 0.496 | 0.025 | 0.446 | 0.378 | 0.471 | 0.190 |
| Subjective P(O|¬ C) | 0.498 | 0.029 | 0.415 | 0.391 | 0.456 | 0.196 |
| Subjective Contingency | −0.002 | 0.029 | 0.031 | 0.156 | 0.014 | 0.081 |
In this experiment, mistakes in the categorizing of outcomes in particular
can be problematic because, if participants are not correctly
understanding what counts as an outcome in a non-ambiguous trial, our
assessment of the interpretation of ambiguous trials could be compromised
and strongly affect our conclusions. Guided by this reasoning, we decided
that an a priori exclusion criterion was necessary: As a result, we
excluded six participants who made more than five mistakes in both cause
and outcome classifications (out of 30 trials) in the whole session, which
could indicate that they either were not paying attention, or did not
understand the instructions. Thus, the final sample consisted of N = 94
participants. Note that an alternative approach is to not exclude any
participant, but including the number of errors as a covariate, which
produces essentially the same conclusions that we report below.
2.2.2 Categorization of ambiguous stimuli
Table 2 depicts the descriptive statistics for the variables assessed in
the experiment: subjective P(O), subjective P(O) conditional on the cause
status (present or absent), and subjective contingency. These were
computed for both ambiguous and non-ambiguous trials.
We have previously described how participants classified the stimuli shown
in non-ambiguous trials. As expected, the task was solvable, and most
participants made no mistakes. This implies that in non-ambiguous trials
the performance was very close to perfect, and the P(O) computed from
these trials is almost a constant in our sample (note the SDs
values are all around zero in Table 2). However, we expected that people
could vary from each other in their interpretation of the stimuli in
ambiguous trials.
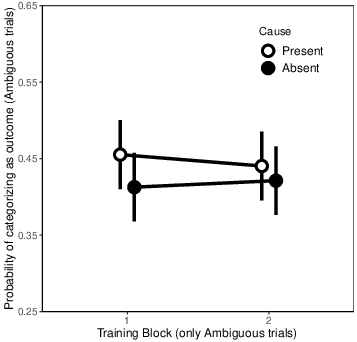
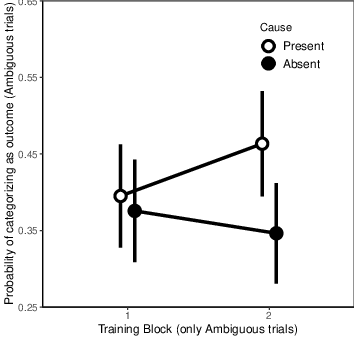
| Figure 4: Probability of categorizing the ambiguous stimulus as “outcome”
for both cause-present and cause-absent trials, divided by training block
(two blocks of 5 trials) in Experiment 1. Error bars depict 95%
confidence intervals for the mean. |
By examining the subjective P(O) for ambiguous stimuli (Table 2), we infer
that the criterion used to categorize these ambiguous stimuli was slightly
conservative, as the mean values were all below 0.50. This means that,
when presented with an ambiguous stimulus, participants tended to classify
it as a non-healed sample of tissue rather than as a healed one. However,
the criterion is still close to 0.50, indicating that this preference in
the classification is small. Additionally, there are no apparent
differences between the probability of reporting an ambiguous stimulus as
a healing in the presence of the cause, P(O|C), and in the
absence of the cause, P(O|¬ C). That is, it seems that people
did not change their classification criterion for ambiguous stimuli as a
function of whether the medicine was taken or not (Table 2, column for
ambiguous trials).
To test these impressions and examine the potential differences in
categorization of ambiguous stimuli depending on whether the cause was
present or not, we conducted a repeated measures 2 (Cause: present/absent)
x 2 (Blocks of 5 trials) ANOVA on the categorization decisions of
ambiguous trials. This resulted in no main effect of Block (F(1,
93) = 0.021, p = 0.885, partial η2
< 0.001), no main effect of Cause (F(1, 93) = 3.301,
p = 0.072, partial η2 = 0.034), and no
interaction (F(1, 93) = 0.533, p = 0.466, partial η2 = 0.006; see Figure 4). In sum, participants
displayed a similar, slightly conservative, criterion to categorize the
ambiguous stimuli in the presence and in the absence of the cause, which
means that they were exposed to very small deviations from the null
contingency. This aligns with the value of subjective contingency for
ambiguous trials, reported in Table 2, which is very close to zero.
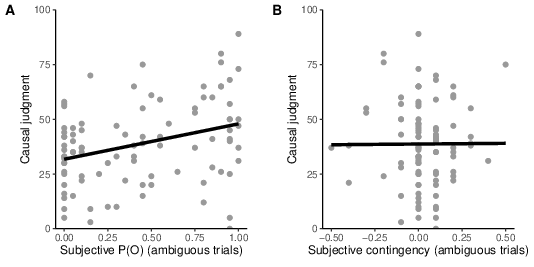
| Figure 5: Scatter plot showing the relationship between causal judgments
and subjective P(O) (computed by taking into account only ambiguous
trials), in Experiment 1. |
2.2.3 Causal judgments
So far, we have described how people classify the stimuli presented in the
task. Now, we test whether individual differences in the categorization of
ambiguous stimuli can predict differences in causal judgments. In
particular, we proposed that those participants with more liberal
classification criteria, and therefore higher values of subjective P(O),
would bias their judgments upwards.
The causal judgments showed some overestimation of the null contingency,
M = 38.71, SD = 18.88. Recall that the actual
contingency that was presented to participants was null, so judgments
higher than zero suggest an overestimation.
Thus, we tested a regression analyses in which the subjective P(O) computed
from ambiguous trials was used as a predictor of judgments. The results
were significant (β = 0.322, t(92) = 3.27, p =
0.002; Figure 5). Moreover, the same effect was found for trials in
which the cause was present and for trials in which the cause was absent,
i.e., P(O|C) and P(O|¬ C) (β = 0.322,
t(92) = 3.27, p = 0.002, and β = 0.309,
t(92) = 3.12, p = 0.002, respectively).
On the other hand, subjective contingency (computed from ambiguous trials)
did not significantly predict the judgments (β = 0.005,
t(92) = 0.050, p = 0.960). This is not surprising, as our
previous analyses showed that most participants tended to categorize
ambiguous stimuli as healings as often in the presence as in the absence
of the cause, that is, they did not seem to take into account whether the
medicine was administered or not in their classification task. As a
consequence, subjective contingency was almost a constant value (very
close to zero) for almost all participants.
The previous analyses were conducted on ambiguous trials only. We have
argued that, because the task of classifying non-ambiguous stimuli was
very easy and the performance close to perfect (furthermore, we excluded
those few participants who made more than five mistakes), values of P(O)
computed from non-ambiguous trials are almost a constant value in our
sample. This means that the variance in the judgments cannot be explained
by these trials, so they add little information. For completeness, we
report here the regression analyses with the P(O) of non-ambiguous trials
only, β = −0.081, t(92) = 0.785, p = 0.435. The
non-significant result suggests that the classification of non-ambiguous
stimuli played no relevant role in the variance of the judgments. If we,
by contrast, repeat the analyses by using all trials (combining ambiguous
and non-ambiguous trials), the results are the same as above with
ambiguous trials only.
3 Experiment 2
Experiment 1 served to illustrate that, when presented with ambiguous
information about an outcome of interest, people can differ in their
tendency to interpret such stimuli as “outcome” or “no outcome”, and that
this tendency can predict a bias in their causal judgments: the more
outcomes the participant has recognized during the task, the stronger the
overestimation of a null contingency. Additionally, we found no evidence
that people make a difference in their categorization of ambiguous
outcomes as a function of whether the potential cause is present or not.
That is, our results favor the hypothesis illustrated in Figure 1a.
However, Experiment 1 was conducted in a null contingency, medium P(C),
medium P(O) setting. In these conditions, we were neither influencing nor
biasing the spontaneous categorization criterion (i.e., there was no
specific incentive to classify the stimuli in a particular way). In
Experiment 2, we go one step further. We propose that the tendency to
categorize outcomes is not fixed, but rather it is context-dependent.
Interestingly, Marsh & Ahn (2009) showed that the categorization of
ambiguous values of a causal cue as “cause” or “no cause” was affected by
the perceived strength of the causal relationship. Thus, we wondered
whether the tendency to categorize ambiguous stimuli as “outcome” could
change if we presented a different situation in non-ambiguous trials: a
positive contingency, instead of a null contingency. In a positive
contingency, the probability of the outcome is higher in cause-present
trials than it is in cause-absent trials. As a result, the categorization
criterion for ambiguous trials could react accordingly, by becoming more
lenient in cause-present trials, and more conservative in cause-absent
trials (this prediction is depicted in Figure 1b). This is due to the
well-known effect of expectations on the classification criterion (Bang &
Rahnev, 2017). The change in the criterion depending on the cause status
would then produce a deviation in the subjective contingency in ambiguous
trials (it would become positive instead of undetermined), and in turn
could exert an effect on causal judgments: the higher the subjective
contingency, the stronger the overestimation. Thus, Experiment 2 was
designed with the aim of testing whether the prediction in Figure 1b is
possible by providing a positive contingency context in the non-ambiguous
trials.
| Table 3: Frequencies of each type of trial in the contingency learning phase in
Experiment 2. |
| | Outcome present (cured) | Ambiguous Outcome | Outcome absent (not cured) |
| Cause present (Medicine was taken) | 14 | 10 | 1 |
| Cause absent (Medicine was not taken) | 1 | 10 | 14 |
3.1 Method
3.1.1 Participants and apparatus.
Forty-one Psychology students (including 4 men) took part in Experiment
2 in exchange for course credit (with age M = 18.60 years,
SD = 1.26), in conditions similar to those of Experiment 1. As
some of the participants were exchange students from other countries,
participants were given the option to choose the language (Spanish,
English) in which they preferred to do the study. All but 4 chose to do
the experiment in Spanish.
3.1.2 Procedure.
The procedure was identical to that of Experiment 1, except for the trial
frequencies (see Table 3). From the numbers of the table, we can compute
P(O|C) = 14/(14+1) = 0.93, and P(O|¬ C) = 1/(1+14)
= 0.07, which yields a contingency of Δ P = 0.86 (a positive, high
value that suggests a strong causal relationship).
3.2 Results and Discussion
| Table 4: Descriptive statistics for the variables in the contingency learning phase
in Experiment 2. |
| | Non-ambiguous trials | Ambiguous trials | All trials |
|
Variable | M | SD | M | SD | M | SD |
| Subjective P(O) | 0.749 | 0.008 | 0.395 | 0.350 | 0.458 | 0.139 |
| Subjective P(O|C) | 0.931 | 0.010 | 0.429 | 0.363 | 0.731 | 0.144 |
| Subjective P(O|¬ C) | 0.067 | 0.000 | 0.361 | 0.353 | 0.184 | 0.141 |
| Subjective Contingency | 0.864 | 0.010 | 0.068 | 0.154 | 0.546 | 0.062 |
3.2.1 Categorization of non-ambiguous stimuli (attention checks).
As in Experiment 1, all participants successfully reached the learning
criterion in the practice phase: 89.5% of participants made no errors in
this phase, while 10.5% made one error, indicating that the
discrimination was correctly acquired. Once in the contingency learning
phase, all but one participant made no mistakes in the outcome
categorization for non-ambiguous trials, and the remaining participant
made only one mistake. Also, as we saw in Experiment 1, categorizing the
cause status produced more errors. In this experiment, 78% of the sample
made no mistakes. No participant made more than five mistakes in their
categorizations of cause and outcome (combined) during the contingency
learning phase, which was our exclusion criterion (the same used in
Experiment 1). Consequently, there were no exclusions in this study.
| Figure 6: Probability of categorizing the ambiguous stimulus as “outcome”
for both cause-present and cause-absent trials, divided by training block
(two blocks of 5 trials) in Experiment 2. Error bars depict 95%
confidence intervals for the mean. |
3.2.2 Categorization of ambiguous stimuli.
We depict the descriptive statistics of the main dependent variables of the
contingency learning phase in Table 4. Given that there were few
categorization mistakes in non-ambiguous trials, the values of subjective
P(O) and subjective contingency in these trials were very close to the
programmed values, with small standard deviations. Thus, we move on to
describing ambiguous trials. Overall, the classification criterion was
conservative in ambiguous trials, as P(O) was lower than 0.50 (i.e.,
participants tended to report ambiguous stimuli as no-outcome, or
non-healed tissue, as in Experiment 1). However, unlike in Experiment 1,
there seems to be a difference in the criterion depending on the cause
status: the probability of reporting an outcome (healing) when classifying
an ambiguous stimulus was higher when the cause was present than when it
was absent, that is, P(O|C) > P(O|¬ C), thus mirroring what
happened in non-ambiguous trials (Table 4). This was confirmed by
statistical analyses: t(40) = 2.84, p = 0.007, d
= 0.443.
To ensure that this difference is reliable, we tested the same model as in
the previous experiment, by conducting a repeated measures 2 (Cause:
present/absent) x 2 (Blocks of 5 trials) ANOVA on the categorization
decisions in ambiguous trials (Figure 6). The main effect of Block was not
significant (F(1, 40) = 0.399, p = 0.531, partial
η2 = 0.01). However, the main effect of Cause was significant
(F(1, 40) = 8.062, p = 0.007, partial η2 = 0.17),
as well as the Block x Cause interaction, F(1, 40) = 4.422,
p = 0.042, partial η2 = 0.10. The interaction can be
interpreted as follows: There is no evidence for differences between
cause-present and cause-absent trials at the beginning of the training
phase (Block 1; t(40) = 0.662, p = 0.512, d =
0.10), but this turns into a significant difference in Block 2
(t(40) = 3.169, p = 0.003, d = 0.495), when the
training has advanced. As expected, this difference is in line with the
positive contingency that was presented in non-ambiguous trials:
participants tended to categorize the ambiguous stimulus as outcome more
often in cause-present trials than in cause-absent trials. This was the
prediction depicted in Figure 1b. Interestingly, the interaction suggests
that this differential criterion depending on the cause status is the
result of learning during the task: in Block 1, the criteria for
cause-present and cause-absent trials are similar to each other and to
those in Experiment 1 (null contingency). However, the exposure to a
positive contingency ends up biasing the criteria to match the contingency.
3.2.3 Causal judgments.
Causal judgments were overall high, M = 58.41 (SD =
19.73), in line with the contingency programmed in non-ambiguous trials
(Δ P = 0.86). Next, we examined the possibility that individual
differences in either subjective P(O) or subjective contingency could
affect the judgments. First, we focused on ambiguous trials only: A
regression analysis showed that, unlike in Experiment 1, subjective P(O)
was not a significant predictor of judgments, β = 0.025,
t(39) = 0.159, p = 0.874. That is, the tendency to
categorize ambiguous stimuli as outcomes did not predict the causal
estimation. Additionally, the subjective contingency measure did not
predict the judgments either, β = 0.026, t(39) = 0.161,
p = 0.873.
In general, it is reasonable that none of the variables predict the causal
judgments, because in this experiment the actual contingency is clearly
positive thanks to the non-ambiguous trials, which makes the contribution
of ambiguous trials to the judgment almost negligible: participants
experienced, if anything, very small divergences from the contingency
programmed in non-ambiguous trials.
The same models were tested for non-ambiguous trials only: subjective
P(O) in non-ambiguous trials did not significantly predict the judgments
(β = 0.068, t(39) = 0.427, p = 0.671); and neither
did subjective contingency (β = 0.068, t(39) = 0.427,
p = 0.671). Remember that there was little variability in these
trials as the classification performance was close to perfect. (Also, the
number of participants is small.) As in Experiment 1, repeating the same
analyses on all trials (by combining ambiguous and non-ambiguous trials)
produces the same result as with ambiguous trials.
4 General Discussion
Individual variability in perceptual abilities or in the tendency to
interpret stimuli could be relevant to improve our understanding of the OD
bias, and perhaps to help us ascertain why some people could be more
vulnerable to its effects. This possibility has not been directly
considered in previous research, to the best of our knowledge. Therefore,
we decided to conduct the two experiments reported here. First, Experiment
1 used a continuous outcome (but presented in a very different fashion
from Chow et al., 2019) in a learning task in which the contingency was
set to zero. That is, the fictitious medicine was unable to make any
change in the healthiness of tissues. Additionally, we also presented
ambiguous trials in which the outcome value was intermediate, thus making
the classification as outcome/no-outcome unsolvable. Participants showed
differences in their tendency to classify these ambiguous trials. These
differences led to variability in the subjective P(O) that they
experienced during the training session, which resulted in higher
judgments of causality for those participants with higher subjective P(O)
values. This is a first demonstration that the OD bias can be intensified
when outcomes are continuous and people display a lenient classification
criterion, thus considering most ambiguous stimuli as outcome occurrences.
Then, in Experiment 2, we explored an additional possibility: that the
tendency to make the categorization is actually the result of learning, or
at least that it is sensitive to the information presented during the task.
Indeed, when we presented a positive, rather than null, contingency
between the cause and the outcome in non-ambiguous trials, participants
ended up developing a differential categorization criterion for ambiguous
trials depending on whether the potential cause was present or not. That
is, they tended to classify ambiguous stimuli as outcome more often in
cause-present trials than in cause-absent trials. This differential
criterion took some time to develop, though, as it appeared only by the
second block of training trials.
It is possible to interpret this change in the classification criterion as
a rational reaction to ambiguous stimuli in positive contingency settings,
rather than as a bias. If participants learn that cause and outcome
(medicine and healing) are positively associated by looking at
non-ambiguous trials, as it happens in Experiment 2, then it makes sense
for them to adjust the criterion for cause-present and cause-absent trials
differentially, to match the probabilities they are being showed in
non-ambiguous trials. Whether rational or biased, this classification
criterion leads to a higher exposure to type a and type d trials, i.e.,
confirmatory evidence, thus increasing the effective contingency
experienced by the participant.
However, whereas in Experiment 1 judgments were consistently predicted by
the subjective P(O), therefore showing an OD bias, in Experiment 2 we
found no evidence for this relationship between P(O) and judgments. In
principle, we would have predicted that either subjective P(O), or
subjective contingency, should predict the judgments in both experiments,
so the results of Experiment 2 are not completely in line with our
expectations. We could interpret this null result in the following way:
since Experiment 2 takes place on a less ambiguous setting (i.e., clearly
positive, rather than null contingency), people’s judgments could be more
directly driven by the information contained in non-ambiguous trials,
leaving too small a room for the interpretation of ambiguous trials to
play a relevant role (i.e., a ceiling effect). In fact, previous research
with the traditional task (binary, easy to discriminate outcomes)
indicated that OD biases are almost always reported, to the best of our
knowledge, with null contingencies. For example, the classic study by
Allan and Jenkins (1980) showed that the overestimation of contingency due
to high levels of P(O) appeared only under null contingency settings, but
not under positive contingency settings. It is possible that judgments in
positive contingency conditions could display a ceiling effect that
prevents the influence of other factors, such as subjective P(O). In sum,
Experiment 2 shows that categorization tendencies can be acquired by
examining contingency, and can become dependent on the cause status (i.e.,
by changing the criterion depending on whether the cause is present), but
does not provide evidence that such tendencies affect judgments in a
positive contingency situation. Future experiments could try to further
investigate this possibility by, perhaps, using lower contingencies for
non-ambiguous trials, thus trying to avoid potential ceiling-effects.
Our current research is one of the few exploring causal learning on
continuous dimensions. Traditionally, contingency learning paradigms show
the information in a discretized format, that is, causes and outcomes can
either be present or absent. Our procedure, by contrast, presents stimuli
that differ along a continuum (from high proportion of dark cells to low
proportion of dark cells). Thus, we can think of outcomes as continuous in
this sense. However, both the cover story and the procedure itself try to
convey the idea that outcomes must be treated as dichotomous. That is, the
participant must make a decision as to whether a given tissue sample is
healed or not. The implication is that there must be a “threshold” in the
outcome continuum that allows a binary classification, and that this
threshold can vary between different participants and conditions. This
allows us to interpret the task in a way that is highly comparable with
most experiments in contingency learning (as, for instance, the rule to
compute contingency stays the same). In sum, although the stimuli that we
used in these experiments can be understood as continuous, in fact the
task worked the same way as in the traditional, binary case.
On the other hand, other experiments have previously tried to study causal
and contingency learning with truly continuous causes and outcomes, and
thus they deserve some comment here. For example, some authors have
investigated causal learning from time series data (Davis et al., 2020;
Soo & Rottman, 2018). In this type of paradigm, participants monitor the
changes and fluctuations of a variable in real time. This variable plays
the role of the outcome, and it could represent anything from the price of
stocks to the hormone levels of a patient. Then, participants are given
the opportunity to intervene on the system (Davis et al., 2020) and see
the effect in real time. Generally, this type of task is known as a
“dynamic system”, because the observed values are non-stationary, so that
contingency becomes hard to assess. Thus, this research deals with a
situation that, although representative of many real-life situations,
departs clearly from the simplistic discrete scenario that we depicted in
the Introduction. Another approach to continuous outcomes that is more
closely related to our research is that developed by Chow et al. (2018),
and that we described above. In Chow et al.’s experiments, the cause
status was binary, as usual in this literature, but outcomes were
presented in numerical format, thus conveying the idea of a continuum.
However, they selected the values of these outcomes so that it was still
possible to set a threshold (albeit arbitrary) to determine, in a binary
fashion, whether the cause was followed by an outcome (i.e., high value)
or not (low value). By making use of this task with continuous outcomes,
Chow et al. (2018) were able to document and replicate the OD bias.
We must mention one caution when interpreting our experiments. Here, we
used unidirectional response scales to collect the judgments, from 0 (the
medicine has no effect) to 100 (the medicine is perfectly effective),
whereas the contingency index Δ P can take on negative values to
represent preventative scenarios. Thus, many researchers advocate
bidirectional scales, from −100 (the medicine is perfectly effective in
worsening the disease) to +100 (the medicine is perfectly effective in
healing the disease). Although it is true that bidirectional scales capture
better the bidirectional nature of contingency, and might change the
participants’ answers (Neunaber & Wasserman, 1986), we argue that they do
not come without problems. To begin with, many participants find it hard to
interpret a bidirectional scale, specially in medical scenarios such as the
one in our experiments (it is difficult to imagine that the medicine
produces the disease). This is probably why unidirectional scales are
popular in the research field of contingency learning. In any case, the
effects studied in these experiments, such as the OD bias, have been
reported both with unidirectional (Musca et al., 2010; Orgaz, Estévez &
Matute, 2013) and bidirectional scales (Perales, Navas, Ruiz de Lara, et
al., 2017; Perales & Shanks, 2003), with almost no substantial differences
(Blanco & Matute, 2020). However, future studies could take into account
the possibility that the type of scale plays a role, by testing and
comparing different scales to each other.
In general, we could interpret our results as a suggestion that, at least
sometimes, there is variability in the way people classify stimuli as
outcomes or no-outcomes by (perhaps) setting arbitrary thresholds in the
stimulus continuum. Then, this variability could produce the OD bias (Chow
et al., 2019). Additionally, people could set a categorization criterion
that aligns with the current causal hypothesis: when one expects the cause
to be effective, the threshold for detecting an outcome occurrence is low
(i.e., lenient criterion) and thus P(O) is inflated, producing a causal
illusion. This process is similar to that described in the perceptual
learning literature, according to which the expectation of a stimulus
affects the detection criterion (Bang & Rahnev, 2017).
On the other hand, a potential limitation in our interpretation of the
results stems from a theoretical view on how people encode the information
contained in events to compute contingency. Here we have assumed that, when
presented with a continuous outcome, participants would parse this
information into a binary discrimination (outcome/no-outcome). In fact,
previous studies suggest that this is the case (Marsh & Ahn, 2009). For
example, Marsh & Ahn (2009) presented participants with a set of different
values for a continuous cause: in one of their stimuli sets, a species of
bacteria that is tall (cause present) was supposed to produce an outcome (a
protein’s presence), whereas a short bacteria was not (cause absent), and
several ambiguous stimuli (mid-height bacteria) were also presented. At the
end of the experiment, people had to recall the number of tall bacteria
they had seen. Their results suggest that people spontaneously dichotomize
the ambiguous values in the continuous dimension of the cause into
categories (tall/short bacteria, or cause present/absent). Additionally,
most theories developed to understand contingency learning assume discrete
categories for causes and outcomes (Beam, 2017; Perales & Shanks, 2007),
as we have mentioned above. However, it is not completely clear whether
this binary categorization is spontaneous on the part of participants or
induced by the task properties (e.g., the way the information
is requested to the participant). In fact, other experiments that
investigated causal learning in dynamic, truly continuous, scenarios,
show that people could effectively learn without apparently needing to
dichotomize the information. Returning to our experiments, if people are
actually capable of capturing and working with continuous events without
discretizing the information, we could not know, since our dependent
variable for assessing categorization was always binary: participants
classified trials as either “outcome-present” or “outcome-absent”, as they
were requested. Therefore, we must remain cautious about the theoretical
implications of the results we report until additional studies are
conducted with different procedures.
These experiments are a first step towards understanding the contribution
to outcome density biases by individual differences in the tendency to
interpret or categorize outcomes. Future studies could investigate further
on the question of how people categorize the stimulus continuum, whether
the categorization can be modulated by external factors (such as
contingencies, prior beliefs...), and how this would affect causal
judgments.
References
Allan, L. G. (1980). A note on measurement of contingency between two
binary variables in judgment tasks. Bulletin of the Psychonomic
Society, 15(3), 147–149. https://doi.org/10.3758/BF03334492.
Allan, L. G., & Jenkins, H. M. (1980). The judgment of contingency and the
nature of the response alternatives. Canadian Journal of
Experimental Psychology, 34(1), 1–11.
https://doi.org/10.1037/h0081013.
Alloy, L. B., & Abramson, L. Y. (1979). Judgment of contingency in
depressed and nondepressed students: sadder but wiser? Journal of
Experimental Psychology: General, 108(4), 441–485.
https://doi.org/10.1037/0096-3445.108.4.441.
Baker, A. G., Mercier, P., Vallée-Tourangeau, F., Frank, R., & Pan, M.
(1993). Selective associations and causality judgments: Presence of a
strong causal factor may reduce judgments of a weaker one. Journal
of Experimental Psychology: Learning, Memory, and Cognition,
19(2), 414–432. https://doi.org/10.1037/0278-7393.19.2.414.
Bang, J. W., & Rahnev, D. (2017). Stimulus expectation alters decision
criterion but not sensory signal in perceptual decision making.
Scientific Reports, 7(1), 1–12.
https://doi.org/10.1038/s41598-017-16885-2.
Beam, C. S. (2017). Models of human causal learning: review,
synthesis, generalization. (A long argument for a short rule). [Doctoral
dissertation, University of Washington]. Washington Research Work Archive.
https://digital.lib.washington.edu/researchworks/bitstream/handle/1773/38679/Beam_washington_0250E_16852.pdf.
Blanco, F., Barberia, I., & Matute, H. (2015). Individuals who believe in
the paranormal expose themselves to biased information and develop more
causal illusions than nonbelievers in the laboratory. PLoS ONE,
10(7), e0131378. https://doi.org/10.1371/journal.pone.0131378.
Blanco, F., Gómez-Fortes, B., & Matute, H. (2018). Causal illusions in the
service of political attitudes in Spain and the United Kingdom.
Frontiers in Psychology, 9, 1033.
https://doi.org/10.3389/fpsyg.2018.01033.
Blanco, F., & Matute, H. (2019). Base-rate expectations modulate the
causal illusion. PLoS ONE, 14(3), e0212615.
https://doi.org/10.1371/journal.pone.0212615.
Blanco, F., & Matute, H. (2020). Diseases that resolve spontaneously can
increase the belief that ineffective treatments work. Social
Science in Medicine, 255, 113012.
https://doi.org/10.1016/j.socscimed.2020.113012.
Blanco, F., Matute, H., & Vadillo, M. A. (2010). Contingency is used to
prepare for outcomes: implications for a functional analysis of learning.
Psychonomic Bulletin & Review, 17(1), 117–121.
https://doi.org/10.3758/PBR.17.1.117.
Buehner, M. J., Cheng, P. W., & Clifford, D. (2003). From covariation to
causation: a test of the assumption of causal power. Journal of
Experimental Psychology. Learning, Memory, and Cognition, 29(6),
1119–1140. https://doi.org/10.1037/0278-7393.29.6.1119.
Byrom, N. C. (2013). Accounting for individual differences in human
associative learning. Frontiers in Psychology, 4, 588.
https://doi.org/10.3389/fpsyg.2013.00588.
Byrom, N. C., & Murphy, R. A. (2017). Individual differences are more than
a Gene x Environment interaction: The role of learning. Journal of
Experimental Psychology: Animal Learning and Cognition, 44(1), 36–55.
Chapman, L. J., Chapman, J. P., & Raulin, M. L. (1976). Scales for
physical and social anhedonia. Journal of Abnormal Psychology,
85(4), 374–382. https://doi.org/10.1037/0021-843X.85.4.374.
Chow, J. Y. L., Colagiuri, B., & Livesey, E. J. (2019). Bridging the
divide between causal illusions in the laboratory and the real world: the
effects of outcome density with a variable continuous outcome.
Cognitive Research: Principles and Implications, 4(1), 1–15.
https://doi.org/10.1186/s41235-018-0149-9.
Eckblad, M., & Chapman, L. J. (1983). Magical ideation as an indicator of
schizotypy. Journal of Consulting and Clinical Psychology,
51(2), 215–225. http://www.ncbi.nlm.nih.gov/pubmed/6841765.
Fonseca-Pedrero, E., Paino, M., Lemos-Giráldez, S., García-Cueto, E., &
Villazón-García, U. (2009). Psychometric properties of the Perceptual
Aberration Scale and the Magical Ideation Scale in Spanish college
students. International Journal of Clinical Health Psychology,
9(2), 299–312.
Griffiths, O., Shehabi, N., Murphy, R. A., & Le Pelley, M. E. (2018).
Superstition predicts perception of illusory control. British
Journal of Psychology, 110, 499–518.. https://doi.org/10.1111/bjop.12344.
Marsh, J. K., & Ahn, W. (2009). Spontaneous Assimilation of Continuous
Values and Temporal Information in Causal Induction. Journal of
Experimental Psychology: Learning, Memory, and Cognition, 35(2),
334–352. https://doi.org/10.1037/a0014929.
Matute, H., Blanco, F., & Díaz-Lago, M. (2019). Learning mechanisms
underlying accurate and biased contingency judgments. Journal of
Experimental Psychology: Animal Learning and Cognition, 45(4),
373–389. https://doi.org/10.1037/xan0000222.
Matute, H., Blanco, F., Yarritu, I., Diaz-Lago, M., Vadillo, M. A., &
Barberia, I. (2015). Illusions of causality: How they bias our everyday
thinking and how they could be reduced. Frontiers in Psychology,
6, 888. https://doi.org/10.3389/fpsyg.2015.00888.
Matute, H., Yarritu, I., & Vadillo, M. A. (2011). Illusions of causality
at the heart of pseudoscience. British Journal of Psychology,
102, 392–405. https://doi.org/10.1348/000712610X532210.
Moreno-Fernández, M. M., Blanco, F., & Matute, H. (2017). Causal illusions
in children when the outcome is frequent. PLoS ONE,
12(9), e0184707. https://doi.org/10.1371/journal.pone.0184707.
Moritz, S., Goritz, A. S., Van Quaquebeke, N., Andreou, C., Jungclaussen,
D., & Peters, M. J. V. (2014). Knowledge corruption for visual perception
in individuals high on paranoia. Psychiatry Research,
215(3), 700–705. https://doi.org/10.1016/j.psychres.2013.12.044.
Moritz, S., Ramdani, N., Klass, H., Andreou, C., Jungclaussen, D., Eifler,
S., Englisch, S., Schirmbeck, F., & Zink, M. (2014). Overconfidence in
incorrect perceptual judgments in patients with schizophrenia.
Schizophrenia Research: Cognition, 1(4), 165–170.
https://doi.org/10.1016/j.scog.2014.09.003.
Moritz, S., Thompson, S., & Andreou, C. (2014). Illusory Control in
Schizophrenia. Journal of Experimental Psychopathology,
5(2), 113–122. https://doi.org/10.5127/jep.036113.
Msetfi, R. M., Murphy, R. A., & Simpson, J. (2007). Depressive realism and
the effect of intertrial interval on judgements of zero, positive, and
negative contingencies. The Quarterly Journal Of Experimental
Psychology, 60(3), 461–481.
https://doi.org/10.1080/17470210601002595.
Musca, S. C., Vadillo, M. A., Blanco, F., & Matute, H. (2010). The role of
cue information in the outcome-density effect: evidence from neural
network simulations and a causal learning experiment. Connection
Science, 22(2), 177–192.
https://doi.org/10.1080/09540091003623797.
Neunaber, D. J., & Wasserman, E. A. (1986). The effects of unidirectional
versus bidirectional rating procedures on college students’ judgments of
response-outcome contingency. Learning and Motivation,
17(2), 162–179. https://doi.org/10.1016/0023-9690(86)90008-1.
Orgaz, C., Estévez, A., & Matute, H. (2013). Pathological gamblers are
more vulnerable to the illusion of control in a standard associative
learning task. Frontiers in Psychology, 4, 306.
https://doi.org/10.3389/fpsyg.2013.00306.
Perales, J. C., Navas, J. F., Ruiz de Lara, C. M., Maldonado, A., &
Catena, A. (2017). Causal learning in gambling disorder: Beyond the
illusion of control. Journal of Gambling Studies, 33(2), 705–717.
https://doi.org/10.1007/s10899-016-9634-6.
Perales, J. C., & Shanks, D. R. (2003). Normative and descriptive accounts
of the influence of power and contingency on causal judgement. The
Quarterly Journal of Experimental Psychology, 56(6), 977–1007.
https://doi.org/10.1080/02724980244000738.
Perales, J. C., & Shanks, D. R. (2007). Models of covariation-based causal
judgment: A review and synthesis. Psychonomic Bulletin & Review,
14(4), 577–596.
Rescorla, R. A. (1968). Probability of shock in the presence and absence of
CS in fear conditioning. Journal of Comparative & Physiological
Psychology, 66(1), 1–5.
Rodríguez-Ferreiro, J., & Barberia, I. (2017). The moral foundations of
illusory correlation. PLoS ONE, 12(10), e0185758.
https://doi.org/10.1371/journal.pone.0185758.
Sauce, B., & Matzel, L. D. (2013). The causes of variation in learning and
behavior: Why individual differences matter. Frontiers in
Psychology, 4, 395. https://doi.org/10.3389/fpsyg.2013.00395.
Shanks, D. R., & Dickinson, A. (1988). Associative accounts of causality
judgment. In G. Bower (Ed.), The Psychology of Learning and
Motivation (Vol. 21, pp. 229–261). Academic Press.
Van Elk, M. (2015). Perceptual biases in relation to paranormal and
conspiracy beliefs. PloS ONE, 10(6), e0130422.
https://doi.org/10.1371/journal.pone.0130422.
Van Elk, M., & Lodder, P. (2018). Experimental Manipulations of Personal
Control do Not Increase Illusory Pattern Perception. Collabra:
Psychology, 4(1), 19. https://doi.org/10.1525/collabra.155.
van Prooijen, J.–W., Douglas, K., & De Inocencio, C. (2017). Connecting
the Dots: Illusory Pattern Perception Predicts Belief in Conspiracies and
the Supernatural. European Journal of Social Psychology,
48, 320–335. https://doi.org/10.1002/ejsp.2331.
Wasserman, E. A. (1990). Detecting response–outcome relations: Toward an
understanding of the causal texture of the environment. In G. H. Bower
(Ed.), The psychology of learning and motivation (Vol. 26, pp.
27–82). Academic Press.
Whitson, J. A., & Galinsky, A. D. (2008). Lacking Control Increases
Illusory Pattern Perception. Science, 322(5898),
115–117. https://doi.org/10.1126/science.1159845.
Yarritu, I., Matute, H., & Luque, D. (2015). The dark side of cognitive
illusions: When an illusory belief interferes with the acquisition of
evidence-based knowledge. British Journal of Psychology,
106(4), 597–608. https://doi.org/10.1111/bjop.12119.
This document was translated from LATEX by
HEVEA.