Judgment and Decision
Making, vol. 2, no. 1, February 2007, pp. 70-78.
On the appropriateness of appropriateness judgments: The case of interferon
treatment for melanoma
Yoav Ganzach1
Faculty of
Management
Tel Aviv University
Moshe Leshno
Sackler Faculty of Medicine and
Faculty of Management
Tel Aviv University
Abstract
We compare experts' judgments of the appropriateness of a
treatment (interferon treatment for melanoma) on the basis of
important attributes of this disease (thickness, ulceration, lymph
node involvement and type of metastases) to a decision analytic
model in which the probabilities of deterioration are derived from
the medical literature and from epidemiological studies. The
comparison is based on what we call the linearity test,
which examines whether appropriateness judgments are a linear
function of the epidemiological value of p2, the probability of
deterioration of the patient condition if he would have received
the treatment. This comparison allows for the assessment of the
validity of the experts' judgments under the assumption that the
decision analytic model is valid, or alternatively, the assessment
of the validity of the decision analytic model under the
assumption that the experts' judgments are valid. Under the former
assumption the results indicate that appropriateness judgments are
by and large accurate. Under the latter assumption the results
support the idea of a constant treatment effect, the idea
that efficacy of a treatment is constant over various levels of
severity of the disease. Our results also support the idea that
experts' aggregate judgments far exceed individuals' judgments.
Keywords: aggregating judgment, medical treatment decisions, decision
analylitic models of judgment, melanoma treatment, ecological validity,
Brunswickian models.
1 Introduction
Appropriateness judgments such as "How appropriate it is to
perform procedure X on a patient with symptoms Y and Z,"
which communicate information of how worthwhile it is to perform
a medical procedure, play a major role in clinical guidelines
systems (Audet, Greenfield, & Field, 1990; Brook, 1994). In
producing such systems, expert clinicians are given scenarios of
a disease (e.g., melanoma) that vary along a number of dimensions
(e.g., size of tumor and number of nodes affected) and are asked
to judge on the appropriateness of using a certain procedure
(e.g., interferon treatment) for each of the cases. These
judgments can later be used by practitioners in deciding whether
or not the treatment should be administered to their patients.
In view of the growing importance of such methods for
communicating expertise in general and medical expertise in
particular (e.g., Field, & Lohr,1990; Shapiro, Lasker, Bindman, &
Lee, 1993) this paper examines
expert appropriateness judgments within the framework of a
normative decision analytic model, evaluates the validity of these
judgments, and assesses their usefulness in understanding clinical
models of treatment. Our empirical work is based on reanalysis of
expert panel judgment that had been used in creating an
authoritative guideline on whether to use interferon as an adjunct
treatment for melanoma.
There are three perspectives from which the relationship between
a decision model and judgments of appropriateness could be
understood. First, if the model is assumed to correctly describe
the judgments, it could be used to uncover the implicit rules, or
policies, underlying these judgments. This is a "policy
capturing" view of judgment modeling (Sheldon, & Kafry, 1997;
Sorum et al., 2002), primarily used to assess attribute weights
in expert judgment, but also to determine the presence of
configural (i.e., interactive) or other nonlinear rules
underlying judgment. Second, if our decision analytic model is
viewed as a prescriptive model of the appropriateness of a
medical treatment, consistency between the model and actual
appropriateness judgments could be viewed as supporting the
validity of those judgments. Third, if a set of appropriateness
judgments are viewed as prescriptively accurate, agreement
between the model and the judgments could be viewed as supporting
the normative stand of the model and the basic tenets on which it
is based. Thus, whereas the second and third perspectives lend
prescriptive status either to the model or to the judgment, the
first perspective is merely descriptive, lending prescriptive
status to neither.
1.1 A decision analytic model for appropriateness
judgments
The term "appropriateness" is the common language analogue of the difference
between the expected utility of taking an action and the expected utility of
not taking that action. Thus, when rating the appropriateness of a treatment
as 6 on a 1 (not appropriate at all) to 9 (very appropriate) scale, the
clinician implies that the expected utility of administering the treatment
is slightly higher than the expected utility of not administering it,
whereas when rating this appropriateness as 9, the clinician implies that
the expected utility of administering this treatment is much higher than the
expected utility of not administering it. It is important to note that
appropriate judgments are intended as a support tool for evaluating the utility
of a treatment. As such, they should serve as a direct (i.e., linear)
indicator of utility, and deviations from linearity should be viewed as
inappropriate. To use an example, consider a panel of experts who are asked
to judge water temperature by sensing the water. Appropriate temperature
judgment in this case should be linearly related to temperature, and the a
linearity test could be viewed as a test of their validity.
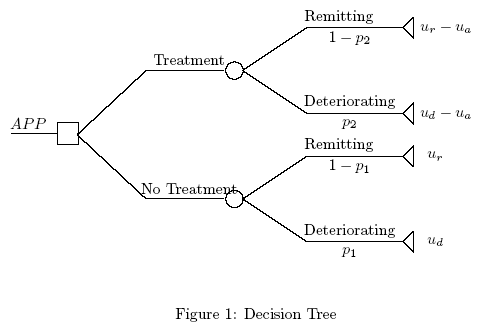
Consider now a clinician's judgment of the appropriateness of a
treatment of a condition that has a probability of p1 of
deteriorating (e.g., death) and 1-p1 of remitting. Assume that
the treatment is associated with probability p2 of
deteriorating p2 < p1 , and a probability 1-p2 of
remitting. Figure 1 depicts the decision tree facing the
clinician. In our model we assume that the probability of adverse
events under treatment equals one. We denote by ur the utility
for remission and ud for deterioration (death). We also assume
that the utility for remission under treatment is equal to ur-ua where ua is the disutility of the adverse event
associated with the treatment2. The expected
utility of administering the treatment (EUT ) and the expected
utility of not administering it (EUNT ) is given by:
|
EUT = p2 (ud -ua )+(1-p2 )(ur -ua ) |
| (1) |
and
|
EUNT = p1 ud +(1-p1 )ur , |
| (2) |
respectively.
Thus, the difference between the expected utility of administering the
treatment (EUT ) and the expected utility of not administering it
(EUNT ) is given by:
If appropriateness judgment is a linear representation of DU=EUT-EUNT (this assumption is further discussed below), then it could be
expressed as:
|
APP=a[ (p2 -p1 )(ud -ur )-ua ] |
| (4) |
where APP represents the level of appropriateness and a
is a positive constant. Denoting p2/p1 = K we obtain
|
APP=a[ p1 (K-1)(ud -ur )-ua ] |
| (5) |
The efficacy of a treatment is defined by [(p1 -p2 )/(p1 )]=1-[(p2 )/(p1 )]=1-1/K. The assumption that p2 /p1=K is constant is
equivalent to asserting that the efficacy of a treatment is
constant over various levels of severity of the disease or that
the effect of the treatment in reducing mortality is constant over
various levels of severity of the disease. For example, if
treatment reduces the probability of mortality of patient A, whose
initial probability of mortality is 0.2, by 10% (to 0.18) it
will also reduce the probability of mortality of patient B, with
an initial probability of 0.8, by 10% (to 0.72). The constant
treatment effect, although not necessarily universally true, may
reasonably describe the effect of treatment in many situations.
This assumption is made in many epidemiological studies. Moreover,
it is mandatory in epidemiological studies where the relative risk
reduction is estimated by regression.
 Whereas our decision analytic model represents appropriateness
judgments as a function of p1, they are usually obtained in
response to clinical scenarios (indications) that include
information about the severity, or levels, of various symptoms.
Therefore, policy capturing studies usually model appropriateness
judgments as a function of the level of symptoms rather than p1
(or any other relevant probabilities) (Kee et al., 2002). This approach has two
disadvantages. First, it does not allow for relating the
descriptive policy capturing model, based on symptoms, to a
prescriptive decision analytic model, based on probabilities and
utilities. Second, the scales of the symptom levels may not be
linear, thus introducing distortion into the interpretation of the
results. In particular, it is not clear whether nonlinear
relationships between the symptom and the judgment represent a
nonlinear clinical rule or nonlinearity in the scale of the
symptoms. To overcome these difficulties, our study models the
judgment in terms of both the "raw" symptom scale and in terms of
a transformed symptom scale in which the levels of the symptom are
expressed using an epidemiological p2 yardstick. For example,
if the severity of the symptom is measured on a 1 (low severity)
to 4 (high severity) scale and the probability of mortality within
five years is, respectively, q1 to q4, then the levels of
the symptoms could be expressed in terms of the probability of
mortality associated with each level, rather than the raw scale
values. This process could be viewed as an intervalization of the
symptom scale. Whereas the raw 1 to 4 scale is not necessarily an
interval scale (equal changes on the scale are not necessarily
equivalent with respect to their impact, e.g., a change from 1 to
2 may differ from a change from 2 to 3), the transformed scale is
interval (equal changes on the scale could be viewed as equivalent
in terms of their impact).
Whereas our decision analytic model represents appropriateness
judgments as a function of p1, they are usually obtained in
response to clinical scenarios (indications) that include
information about the severity, or levels, of various symptoms.
Therefore, policy capturing studies usually model appropriateness
judgments as a function of the level of symptoms rather than p1
(or any other relevant probabilities) (Kee et al., 2002). This approach has two
disadvantages. First, it does not allow for relating the
descriptive policy capturing model, based on symptoms, to a
prescriptive decision analytic model, based on probabilities and
utilities. Second, the scales of the symptom levels may not be
linear, thus introducing distortion into the interpretation of the
results. In particular, it is not clear whether nonlinear
relationships between the symptom and the judgment represent a
nonlinear clinical rule or nonlinearity in the scale of the
symptoms. To overcome these difficulties, our study models the
judgment in terms of both the "raw" symptom scale and in terms of
a transformed symptom scale in which the levels of the symptom are
expressed using an epidemiological p2 yardstick. For example,
if the severity of the symptom is measured on a 1 (low severity)
to 4 (high severity) scale and the probability of mortality within
five years is, respectively, q1 to q4, then the levels of
the symptoms could be expressed in terms of the probability of
mortality associated with each level, rather than the raw scale
values. This process could be viewed as an intervalization of the
symptom scale. Whereas the raw 1 to 4 scale is not necessarily an
interval scale (equal changes on the scale are not necessarily
equivalent with respect to their impact, e.g., a change from 1 to
2 may differ from a change from 2 to 3), the transformed scale is
interval (equal changes on the scale could be viewed as equivalent
in terms of their impact).
1.2 On the validity of appropriateness judgments
Assessment of validity in medical judgments has taken primarily
either the approach of comparing methods (Bosch, Halpern, &
Gazelle, 2002; Shackman et al., 2002), or examining whether the
decision process suffers from biases (Chapman, & Sonnenberg,
2000; Stalmeier, 2002). A few studies have also examined the
validity of appropriateness judgments by comparing them to
normative models (Kuntz, Tsevat, Weinstein, & Goldman, 1999;
Bernstein, Hofer, Meijler, & Rigter, 1997). In contrast to these
approaches, our basic test for the validity of appropriateness
judgments is based on a Brunswickian approach of comparing the
function form in the environment model - the model that predicts the
criterion from the cues - to the function form in the judgment
model - the model that predicts the judgments from the cues
(e.g., Stewart & Joyce, 1988, Wigton, 1996). In particular, our
test, labeled the linearity test, involves an
examination whether, in agreement with the model, appropriateness
judgments are a linear function of the epidemiological value of
p1 (the probability derived from epidemiological studies). The
linearity test is a test of the validity of appropriateness
judgments, since to the extent that our decision analytic model
is a correct model of appropriateness, valid judgments should
satisfy this test. Thus, a linear relation supports (though it
does not prove) the validity of appropriateness judgments,
whereas a nonlinear relation provides some evidence against their
validity. Note however that a nonlinear relationship does not
necessarily suggest that appropriateness judgments are not valid.
In particular, nonlinearity may be the result of our model being
normatively incorrect (e.g., the assumption of a constant
treatment effect is incorrect) rather than the appropriateness
judgments being incorrect (e.g., judgments that rely on erroneous
assessment of probability or utility, or on a correct integration
of the two). Thus, our linearity test could be viewed as a joint
test of the validity of our model for appropriateness judgment
and the validity of the judgments themselves. Both need to be
valid for linearity to occur.
1.3 The validity of individual judgments vs. the
validity of the aggregated judgments
A basic question in medical decision making is whether aggregating the
judgments of clinicians result in more valid clinical judgments. Despite the
fundamental importance of this question, not much relevant empirical
evidence is available, primarily because of problems associated with the
establishment of criteria that will allow the evaluation of the utility of
the aggregation.
In the context of the current study, a criterion for the
evaluation of the utility of the aggregation is available -
whether or not judgments are linear. Thus our empirical test for
the utility of aggregation of clinical judgments is whether or not
the aggregated judgments conform with the linearity test better
than the individual judgments.
1.4 The validity of expected utility models of treatment
and the constant treatment effect hypothesis
Our discussion so far has focused on the validation of
appropriateness judgments under the assumption that our decision
analytic model is a valid model of the appropriateness of a
medical treatment. However, as mentioned earlier, a complementary
perspective emphasizes the validation of the model under the
assumption that the appropriateness judgments are valid. In
particular, if appropriateness judgments are assumed to be
normatively valid and linearity is satisfied, the assumption of a
constant treatment effect is supported.
1.5 Interferon treatment for malignant melanoma
In this study we examine the validity of appropriateness judgments
in a specific clinical setting, adjuvant high-dose interferon
alfa-2b in treating melanoma. Malignant melanoma is a common
cancer in the western world. During the last 20 years, numerous
agents have been evaluated in a series of both nonrandomized and
randomized adjuvant therapy trials in melanoma. For patients who
are in advanced stages of malignant melanoma, controversy abounds
regarding high-dose adjuvant interferon alfa-2b therapy. Based on
randomized clinical trials, it is currently agreed that high-dose
interferon therapy is associated with approximately 10%
improvement in relapse-free survival but also with high incidence
of serious toxicity (Schuchter, 2004). In other words, relapse-free
survival is "bought" at the price of increased frequency of
serious toxicity. So the appropriateness judgments must revolve
around the perceived tradeoff between harms and benefits.
2 Method
The judgments analyzed in this study were appropriateness
judgments of high-dose interferon treatment of melanoma collected
by Dubois et al. (2001) elicited from a panel of 13 experts
(four dermatologists, four oncologist and five surgeons) using
the RAND Delphi method (Park et al., 1986; Landrum & Normand,
1999). The judgments were given in response to 56 clinical
scenarios based on permutations of four factors: thickness of the
tumor, classified into four levels, level 1 ( £ 1.00 mm),
level 2 (1.01-2.00 mm), level 3 (2.01-4.00 mm) and level 4
( > 4.0 mm); ulceration (present or absent); LNI, or lymph node
involvement - the number of lymph nodes to which the tumor had
spread (none, 1, 2, 3, or ³ 4); and presence of micro
metastases vs. macro metastases (for patients with LNI > 0).
The judgments were given on a 9-point scale where 9 indicated
extremely appropriate, 5 uncertain and 1 extremely inappropriate.
Appropriateness was defined as "the expected health benefits of
the therapy exceeding its expected negative health consequences by
a sufficiently wide margin to justify giving the therapy"
(Averbook et al., p. 1218), suggesting a difference model (e.g.,
Anderson, 1990; Rule, Curtis & Mullin, 1981).
Our analysis will focus on the effect of tumor thickness on
judgment because of its central role in estimating the prognosis
of primary melanoma in the clinical literature.3 (Balch
et al., 2000), and because good epidemiological
data regarding this effect are available, in contrast to the lack
of such data regarding the effect of LNI and ulceration. Our
epidemiological source supplies a univariate probability of
mortality for each level of thickness, but provides the
probability of mortality only for a present/absent dichotomy with
regard to LNI and ulceration and no data regarding presence of
metastasis.
Our estimate of p1 (the probability of deterioration given
treatment) was based on the literature. In a recent
epidemiological study (Averbook et al., 2002) p1 of melanoma
patients was reported as a function of thickness, (p1
approximately equal to 0.1, 0.2, 0.4 and 0.65, respectively, for
levels 1 through 4), LNI (p1 is 0.447 when there is node
involvement and 0.117 when there is no node involvement) and
ulceration (p1 is 0.443 when there is ulceration and 0.129
when there is no ulceration).
3 Results
We first analyzed the mean appropriateness judgments of the 13
panelists. We began by examining the correlations between the
average appropriateness judgment and the severity of each symptom
(aggregated over the levels of the symptoms and averaged over
judges). Since by design the association between the symptoms was
negligible, these correlations reflect the weight each symptom
has in the judgment. (For linear relationships between the
judgments and symptom, these correlations are a precise
representation of the weight. For nonlinear but monotonic
relations they are an approximate, yet good, representation of
these weights.) The values of the correlations are 0.68, 0.23
0.07 and 0.48 for LNI, thickness, ulceration, and presence of
metastasis, respectively.4
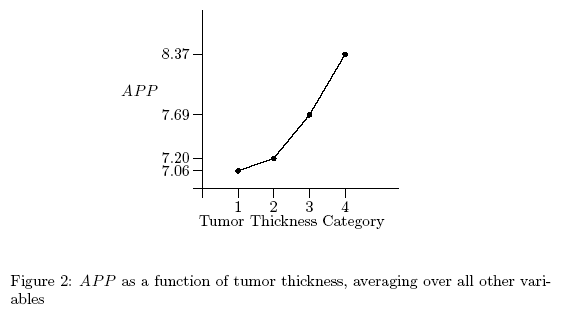
Figure 2 presents the average aggregated appropriateness judgments (aggregated over
the various levels of LNI and ulceration and averaged over judges) as a
function of thickness, using the original "raw" 1-4 thickness scale. This
figure suggests that the relationship between raw thickness and
appropriateness judgment is not linear. Indeed, the functional relationship
between the level of thickness and the average ratings of the 13 judges
differed significantly from a linear function (p < 0.005).
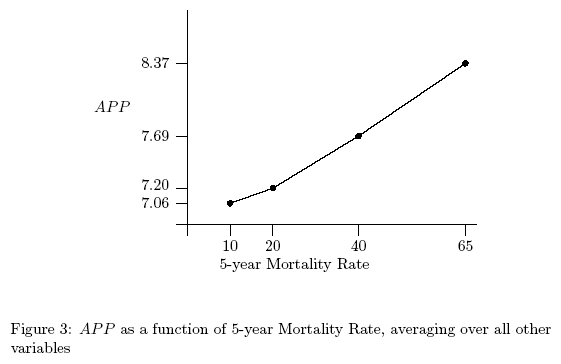
 However, an appropriate test of linearity requires transforming raw
thickness into an interval scale by positioning each level of thickness on a
scale of probability of mortality, as estimated from epidemiological data
(see above). This is presented in Figure 3. It is clear from this figure
that on an interval thickness scale the relationship between thickness and
the average aggregated appropriateness judgment is linear. Indeed, the
functional relationship between the level of thickness after transformation
and the average ratings of the 13 judges does not differ significantly from
a linear function (p > 0.2). Thus, the linearity test is satisfied in our
data.
However, an appropriate test of linearity requires transforming raw
thickness into an interval scale by positioning each level of thickness on a
scale of probability of mortality, as estimated from epidemiological data
(see above). This is presented in Figure 3. It is clear from this figure
that on an interval thickness scale the relationship between thickness and
the average aggregated appropriateness judgment is linear. Indeed, the
functional relationship between the level of thickness after transformation
and the average ratings of the 13 judges does not differ significantly from
a linear function (p > 0.2). Thus, the linearity test is satisfied in our
data.
 Figures 4 and 5 present the individual aggregated judgments of the
13 judges (aggregated over the various levels of LNI and
ulceration). By comparing Figures 4 and 5 to Figure 3, it is clear
that the average appropriateness judgments are more linear than
the individual appropriateness judgments. Out of the 13 judges,
only four exhibit a linear relationship between judged
appropriateness and the 5-year mortality rate as proposed by the
analytical decision model - the other exhibit either marginally
decreasing or marginally increasing functions. However, the
average appropriateness rating of all the judges revealed a linear
relationship between the appropriateness and the 5-year mortality
rate.
Figures 4 and 5 present the individual aggregated judgments of the
13 judges (aggregated over the various levels of LNI and
ulceration). By comparing Figures 4 and 5 to Figure 3, it is clear
that the average appropriateness judgments are more linear than
the individual appropriateness judgments. Out of the 13 judges,
only four exhibit a linear relationship between judged
appropriateness and the 5-year mortality rate as proposed by the
analytical decision model - the other exhibit either marginally
decreasing or marginally increasing functions. However, the
average appropriateness rating of all the judges revealed a linear
relationship between the appropriateness and the 5-year mortality
rate.
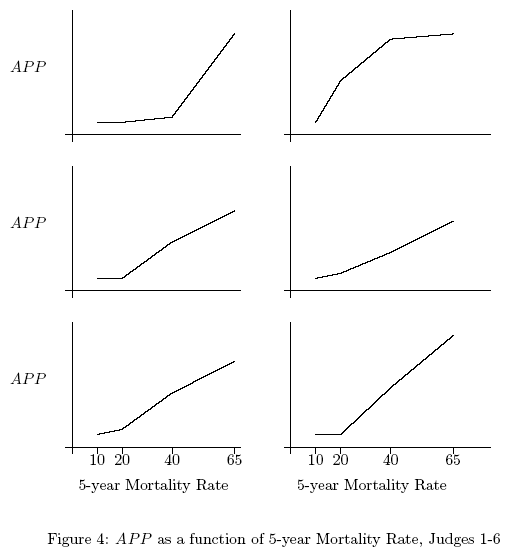
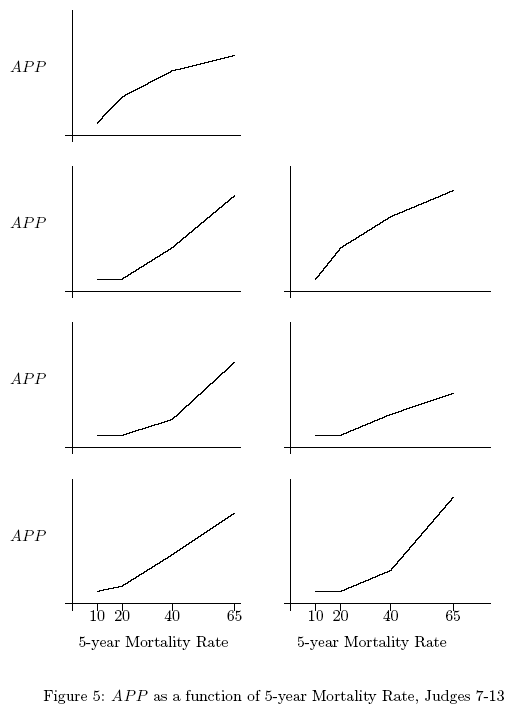 Figure 6 presents the average appropriateness judgment
as a function of thickness separately for each level of
LNI (in this figure the judgments are aggregated only over the
two levels of ulceration and averaged over the 13 judges). In
Figure 6 the thickness scale is the original raw scale whereas
in Figure 7 it is the transformed interval scale. One thing that
is apparent from this figure is that, whereas raw thickness is
not linearly related to appropriateness judgment within each
level of LNI, after transformation, thickness is linearly related
to these judgments within each of these levels. This finding is
consistent with the idea that our transformation of raw thickness
results in an interval thickness scale.5
Figure 6 presents the average appropriateness judgment
as a function of thickness separately for each level of
LNI (in this figure the judgments are aggregated only over the
two levels of ulceration and averaged over the 13 judges). In
Figure 6 the thickness scale is the original raw scale whereas
in Figure 7 it is the transformed interval scale. One thing that
is apparent from this figure is that, whereas raw thickness is
not linearly related to appropriateness judgment within each
level of LNI, after transformation, thickness is linearly related
to these judgments within each of these levels. This finding is
consistent with the idea that our transformation of raw thickness
results in an interval thickness scale.5
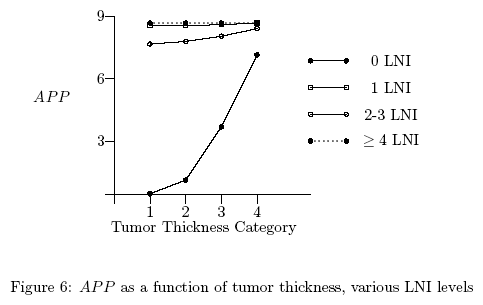
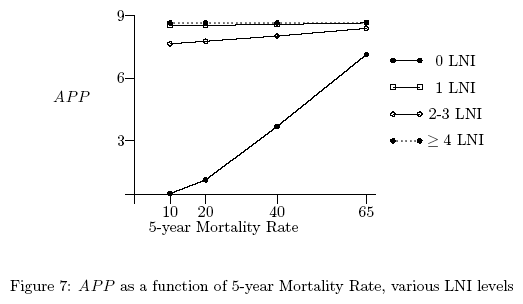 Finally, both Figures 6 and 7 suggest that the relationship
between thickness, LNI and appropriateness judgment is
disjunctive: thickness has a larger impact on appropriateness
when the LNI level is low than when it is high (repeated measures
ANOVA with thickness and LNI as repeated measures revealed a
significant interaction between the two, F(1,108) = 108.9,
p < 0.0001). This pattern is consistent with a policy in which
once the evidence for a severe malignancy pass a certain
threshold, treatment is universally recommended.6
Finally, both Figures 6 and 7 suggest that the relationship
between thickness, LNI and appropriateness judgment is
disjunctive: thickness has a larger impact on appropriateness
when the LNI level is low than when it is high (repeated measures
ANOVA with thickness and LNI as repeated measures revealed a
significant interaction between the two, F(1,108) = 108.9,
p < 0.0001). This pattern is consistent with a policy in which
once the evidence for a severe malignancy pass a certain
threshold, treatment is universally recommended.6
4 Discussion
In this section we first discuss the results from the point of
view of the three perspectives by which the relationship between
our decision analytic model and the judgments of appropriateness
could be understood. The first perspective, the policy capturing
perspective, suggests that, if the model is assumed to correctly
describe the judgment, insight regarding the implicit rules
underlying the judgment could be revealed. Indeed two such
insights are revealed by our analysis. First, the analysis
reveals a discrepancy between the epidemiological data regarding
the importance of LNI and thickness reported by Averbook et
al. (2002) and the subjective weights assigned to these factors
by the judges. According to the Averbook et al. (2002) data,
thickness is the most important determinant of p1, whereas
according to the judgments, LNI is the most important
characteristic of p1. Second, the analysis reveals a configural
(disjunctive) rule with respect to the integration of the
severity of thickness and severity of LNI in the determination of
appropriateness, in that thickness has a larger impact on
appropriateness when the level of LNI is low than when it is
high.
The second perspective suggests that, if our decision analytic model is a
prescriptive model of the appropriateness of a medical treatment,
consistency between the model and appropriateness judgment could be viewed
as supporting the validity of the judgment. Within this context it is
worthwhile to distinguish between three types of validity of appropriateness
judgment. Ecological validity refers to valid perception of the
probabilities (and utilities7) associated with the judgment. Normative validity
refers to reliance on normative rules (e.g., rules for integrating
probabilities and utilities) in arriving at a judgment. Scale validity
refers to accurate use of judgment scales, in our case valid use of the
appropriateness scale, and in particular to the notion that appropriateness
judgments are a linear representation of the difference between subjective
expected utility of treatment versus no-treatment. Although none of these
three validities is directly demonstrated by the results, they are all
supported by the data, since all are necessary for appropriateness judgment
to be a linear function of thickness under the assumption that the decision
analytic model is valid.
The third perspective suggests that, if appropriateness judgments are viewed
as prescriptively accurate, a consistency between the model and the
judgments could be viewed as supporting the prescriptive stand of the model
and the basic tenets on which it is based, in particular the assumption of
constant treatment effect.
It is important to note that the constant treatment effect
stipulates linearity between appropriateness judgment and
thickness only with regard to the average (over the various
levels of the other symptoms) appropriateness judgment. It does
not necessarily stipulate linearity between thickness and
appropriate judgments at each level of LNI. The latter
requirement, labeled multivariate linearity, is weaker than the
former, labeled univariate linearity. In fact, multivariate
linearity is a sufficient but not necessary condition for
univariate linearity. Conceptually, the difference between the
two types of linearity is that whereas univariate linearity
suggests that the effect of interferon treatment does not depend
on the severity of the melanoma, multivariate linearity suggest
that, other things being equal, the effect of interferon
treatment is constant for various levels of thickness.8
Within this context, note that the difference in slopes of the
effect of thickness on the appropriateness of interferon treatment
is explained in terms of different values of K for various
levels of node involvement. A larger slope for high node
involvement than for low node involvement will occur if
K=p2/p1 is larger for high node involvement than for low node
involvement; that is, if the effect of treatment is generally
(e.g., across levels of thickness) higher for high node
involvement than for low node involvement.
One particular interesting aspect of our analysis is the comparison between
the individual judgments and the average judgments. Assuming that the
average judgments represent a "true" model of the medical community's view
of the relationship between the symptom (thickness) and the appropriateness
of interferon treatment, deviations from these judgments - or for that
matter deviation from linearity - could be viewed as an error. There are
two plausible sources for this error. First, it could stem from an
individual judge's idiosyncratic models, dissimilar to the clinical
community's mode. And second, it could stem from a random noise. The
systematic nature of the individual judges' deviations from linearity (i.e.,
the deviations are either marginally decreasing or marginally increasing) is
consistent with a systematic, but not with a random, deviation from the true
model. In particular, our analysis of the individual judgments (Figures 4
and 5) suggest two types of idiosyncratic models underlying judges
systematic errors, a marginally increasing model associated with a threshold
above which increase in probability does not lead to much change in
appropriateness, and a marginally decreasing model associated with a
threshold below which increase in probability does not lead to much change
in appropriateness.
Another explanation for the individual judges' deviations from linearity is
nonlinearity in the appropriateness scale. Within this context it is
important to note that appropriate judgments are aimed as a support tool to
help rank and file physicians evaluate the utility of a treatment. As such
they should serve as a direct (i.e. linear) indicator of utility, and
deviations from linearity should be viewed as inappropriate. To use an
example, consider a panel of experts who are asked to judge water
temperature by sensing the water. Appropriate temperature judgment in this
case should be linearly related to temperature, and the a linearity test
could be viewed as a test for their validity.
What are the implications of this study for the status of appropriateness
judgments in medical decision making? By and large, the results of the study
highlight the importance of combining the clinical judgments of individual
experts, and strengthen our confidence in the appropriateness of averaged
appropriateness judgments. The appropriateness judgments examined in this
study, which is based on averaged or consensus judgments, appear to be valid
in that they reflect accurate perception of probabilities, reliance on
normative strategies in incorporating these probabilities into clinical
evaluation, and adequate expression of this evaluation in manifested
judgment (i.e., in an appropriateness scale). Furthermore, our results also
highlight the utility of aggregation over judges, since the average
judgments are more linear than the individual judgments, which, in terms of
our model, implies better judgment. (This finding is consistent with
Goldberg, 1970. See also Hammond, Hamm, & Grassia, 1986).
Second, the study provides an example of how the analysis of appropriateness
judgments can be used to capture clinical intuition, by revealing the
implicit rules underlying clinical judgment about treatment effects. In our
case, the analysis of these judgments suggests rules such as the constant
treatment effect in its univariate and multivariate forms, and shifts in the
judged effectiveness of treatment at various levels of LNI.
Finally, the lack of linearity in the thickness scale raises a question
regarding the appropriateness of the scales by which medical information is
communicated to clinicians in general and to experts making appropriateness
judgments in particular. Nonlinearity of a symptom scale is an undesirable
feature, since, in comparison to a linear scale, it does not permit the
natural assessment of the implications of clinical information for
treatment. Thus, even though moving from simple, non-epidemiological, scales
(such as length in millimeters for thickness) is cumbersome, a stronger
emphasis on the construction of linear, or interval, scales based on
epidemiological information seems a desirable direction for improved
communication of clinical information.
References
Anderson, N. H. (1990).
Contributions to information integration theory, Vol. 1:
Cognition.
Hillsdale, NJ: Lawrence Erlbaum Associates, Inc.
Audet, A. M., Greenfield S. and Field M. (1990).
Medical practice guidelines:current activities and future directions.
Annals of Internal Medicine, 113, 709-714.
Averbook, B. J. Fu P., Rao, J. S. and Mansour, E. G. (2002).
A long term analysis of 1018 patients with melanoma by classic cox
regression and tree-structured survival analysis at a major referral center:
Implications for the future of cancer staging.
Surgery, 132, 589-604.
Balch, C. M. Buzaid, A. C. Atkins, M. B. et al. (2000).
A new ajcc staging system for cutaneous melanoma.
Cancer, 88, 1484-1491.
Balch, C. M. Soong, S. J. Gershenwald, J. E. Thompson, JF. et al. (2001).
Prognostic factors analysis of 17,600 melanoma patients: validation
of the american joint committee on cancer melanoma staging system.
Journal of Clinical Oncology, 19, 3622-3634.
Bernstein, S. J. Hofer, T. P. Meijler, A. P. and Rigter H. (1997).
Setting standards for effectiveness: a comparison of expert panels
and decision analysis.
International Journal for Quality in Health Care, 9, 255-263.
Bosch, J. L., Halpern, E. F. and Gazelle, G. S. (2002).
Comparison of preference-based utilities of the short-form 36 health
survey and health utilities index before and after treatment of patients with
intermittent caludication.
Medical Decision Making, 22, 403-409.
Brook, R. H. (1994).
Appropriateness: The next frontier [editorial].
BMJ, 308, 218-219.
Chapman, G. B. and Sonnenberg FA. (Eds). (2000).
Decision making in health care: Theory, psychology, and
applications, volume 22.
Cambridge University Press.
Dubois, R. W. Swetter, S. M. Atkins M. McMasters, K. et al. (2001).
Developing indications for the use of sentinel lymph node biopsy and
adjuvant high-dose interferon alfa-2b in melanoma.
Archives of Dermatology, 137, 1217-1224.
Field, M. J. and Lohr, KN. eds. (1990).
Clinical Practice Guidlines: Directions for a New Agency:
Institute of Medicienc.
Washington, DC: National Acacemy Press.
Goldberg, L. W. (1970).
Man versus model of man: A rationale plus
some evidence for a method of improving on clinical inference.
Psychological Bulletin, 73, 422-432.
Hammond, K. R., Hamm, R. M., & Grassia, J. (1986).
Generalizing over conditions by combining the multitrait-multimethod matrix and the
representative design of experiments.
Psychological Bulletin, 100, 257-269.
Kee F. Patterson, C. C. Wilson, A. E. McConnell J. M. et al. (2002).
Judgment analysis of prioritization decision within a dialysis
program in one united kngdom region.
Medical Decision Making, 22, 140-151.
Kuntz, K. M. Tsevat J. Weinstein, M. C. and Goldman L. (1999).
Expert panet vs decision -analysis recommendations for postdischarge
coronary angiography after myocardial infarction.
JAMA, 282, 2246-2251.
Landrum, M. B. Normand, S. L. (1999).
Applying bayesian ideas to the development of medical guidelines.
Statistics in Medicine, 18, 117-137.
Park, R. E. Fink A. Brook, R. H. Chassin MR. et al. (1986).
Physician ratings of appropriate indications for sixe mecical and
surgical procedures.
American Journal of Public Health, 76, 766-772.
Rule, S. J. Curtis, D. W and Mullin, L. C. (1981).
Subjective ratios and differences in perceived heaviness.
Journal of Experimental Psychology: General, 7, 459-466.
Schuchter, L. M. (2004).
Adjuvant interferon therapy for melanoma: High-dose, low-dose,
no-dose, which dose?
Journal of Clinical Oncology, 22, 7-10.
Shackman, B. R. Goldie, S. J. Freedberg, K. A. Losina E. et al. (2002).
Comparison of health state utilities using community and patients
preference weights derived from survey of patients with hiv/aids.
Medical Decision Making, 22, 27-38.
Shapiro, D. W. Lasker, R. D. Bindman, A. B and Lee, P. R. (1993).
Containing costs while improving quality of care: the role of
profiling and practice guidelines.
Annual Review of Public Health, 14, 219-241.
Sheldon Z. and Kafry D. (1997).
Capturing rater policies for processing evaluation data.
Organizational Behavior and Human Performance, 18, 269-294.
Sorum, P. C., Stewart, T. R., Mullet E., González-Vallejo, C.,
et al. (2002). Does choosing a treatment depend on making a
diagnosis? US and french physicians' decision making about acute
otitis media. Medical Decision Making, 22, 394-402.
Stalmeier, P. F. (2002).
Discrepancies between chained and classic utilities induced by
anchoring and occasional adjustment.
Medical Decision Making, 22, 53-64.
Stewart, T. R., & Joyce, C. R. B. (1998).
Increasing the power of clinical trials through judgment analysis.
Medical Decision Making, 8, 33-38.
Wigton, R. S. (1996).
Social judgment theory and medical judgment.
Thinking and Reasoning, 2, 175-190.
Footnotes:
1Mailing Address: Yoav Ganzach, Faculty of Management, Tel Aviv University,
Tel Aviv 69978 Israel, Tel: +972-3-6406467, Fax: +972-3-6046982,
E-mail:yoavgn@post.tau.ac.il.
2This assumption suggests a
fixed treatment protocol, e.g., independence of the treatment on
p2 . This, indeed is the case in interferon treatment (where
the dose of the treatment depends only on the surface area of the
patients and not on the severity of the disease).
3For
example (Balch et al., 2001), "... it is well
established that tumor thickness is the single most important
prognostic feature of primary melanoma."
4For presence for metastasis
the correlation was performed only within the scenarios for
which there was lymph node involvement.
5Note that in
Figure 6 - unlike Figure 2 - the abscissa cannot be
interpreted as a probability scale, and therefore linearity in
each of the node levels is not directly associated with our
decision analytic model. Note also that linearity between
appropriateness judgments and symptom A (i.e., thickness) for
each level of symptom B (i.e., number of nodes) is a sufficient
condition for linearity between appropriateness judgments and
symptom A on the aggregate level.
6Note
that because of the crossing of the simuli in the design, the
averages over other values of the cues and over LNI in
particular, lead to a linear function in thickness, even though
the multi-cue pattern is disjunctive
7Note, however, that our data are only
relevant to testing the valid perception of probabilities. Furthermore, the
test of valid perception of utilities is much more ambiguous since utilities
vary across people.
8To
see why multivariate linearity is not necessary for univariate
linearity consider a case in which the relationship between the
level of symptom A and appropriateness is marginally increasing
at one level of symptom B and marginally decreasing at another
level of this symptom. This could lead to univariate linearity
in regard to A, associated with multivariate
nonlinearity.
File translated from
TEX
by
TTH,
version 3.74.
On 9 Feb 2007, 06:10.