Jorge-Eduardo Martinez-Perez
University of Murcia
Murcia, Spain
José-María Abellán-Perpiñán
University of Murcia
Murcia, Spain
Keywords: framing effect, risk format, standard gamble, health state, dual-process theories.
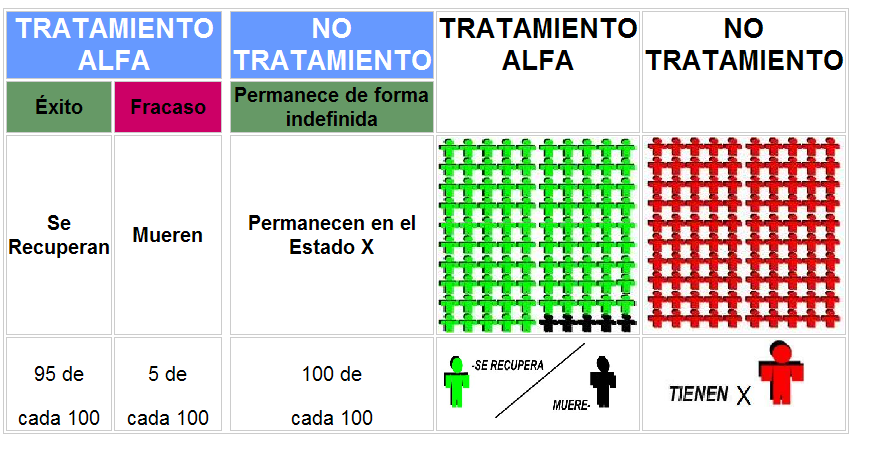
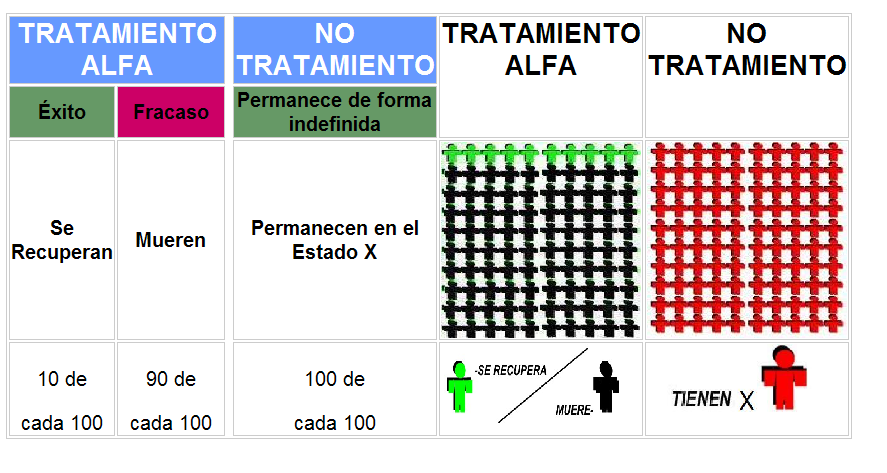
| (1) |
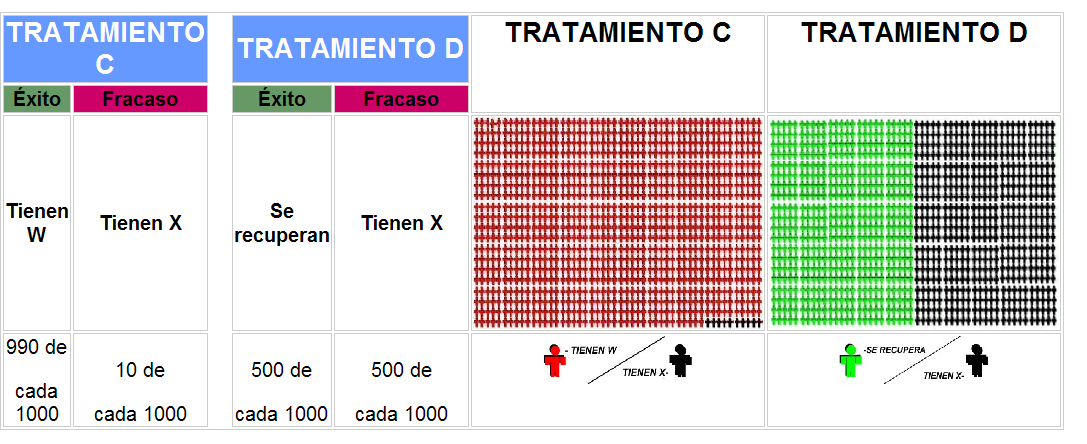
| Health state X (22111): Some problems walking about Some problems with performing self care activities (e.g., eating, washing or dressing) No problems with performing usual activities (e.g., work, study, housework, family or leisure activities) No pain or discomfort Not anxious or depressed | Health state W (11222): No problems walking about No problems with performing self care activities (e.g., eating, washing or dressing) Some problems with performing usual activities (e.g., work, study, housework, family or leisure activities) Moderate pain or discomfort Moderately anxious or depressed |
| Health state Z (22222): Some problems walking about Some problems with performing self care activities (e.g., eating, washing or dressing) Some problems with performing usual activities (e.g., work, study, housework, family or leisure activities) Moderate pain or discomfort Moderately anxious or depressed | Health state Y (23222): Some problems walking about Unable to wash or dress self Some problems with performing usual activities (e.g., work, study, housework, family or leisure activities) Moderate pain or discomfort Moderately anxious or depressed |
| Health state X | Health state W | Health state Z | Health state Y | |||||
| Group: | N100 | N1000 | N100 | N1000 | N100 | N1000 | N100 | N1000 |
| Median | 60.00 | 60.00 | 60.00 | 50.00 | 30.00 | 30.00 | 15.00 | 12.50 |
| Mean | 57.32 | 61.10 | 56.23 | 53.75 | 30.56 | 30.15 | 16.62 | 16.51 |
| (SD) | (1.66) | (1.57) | (1.49) | (1.47) | (0.95) | (1.17) | (0.82) | (0.94) |
| Health state X** | Health state W** | Health state Z* | Health state Y* | |||||
| Group | N100 | N1000 | N100 | N1000 | N100 | N1000 | N100 | N1000 |
| Median | 0.850 | 0.945 | 0.800 | 0.908 | 0.600 | 0.700 | 0.375 | 0.500 |
| Mean | 0.790 | 0.902 | 0.796 | 0.880 | 0.575 | 0.673 | 0.393 | 0.481 |
| (SD) | (0.185) | (0.105) | (0.161) | (0.120) | (0.271) | (0.232) | (0.272) | (0.313) |
| U1000-U100 (from means) | 0.112 | 0.084 | 0.098 | 0.088 | ||||
| (1-U1000)/(1-U100) | 0.47 | 0.59 | 0.77 | 0.86 | ||||
| * Significant different at a=0.05 using t-test and Wilcoxon Mann-Whitney test. | ||||||||
| Injury X: | Injury W: |
In hospital.
| In hospital
|
| Group A | Group B | |||||
| (lr)2-3(lr)4-5 Risk | Mean | Median | Mean | Median | T-test | U-test |
| r | 15.2 out of 1000 | 5 out of 1000 | 14.8 out of 1000 | 5 out of 1000 | 0.911 | 0.120 |
| q | 37.1 out of 100 | 33.5 out of 100 | 176 out of 1000 | 95 out of 1000 | 0.000 | 0.000 |